Pregnancy outcomes in twin pregnancies over 10 years
Article information
Abstract
Objective
The aim of this study was to evaluate the changes in twin pregnancy outcomes between 2007 and 2016 in a Korean population.
Methods
The data for this nationwide population-based study was obtained from the national birth registry of the Korean National Statistical Office and the Health Insurance Review & Assessment Service of Korea. Women with twin pregnancies who gave birth between 2007 and 2016 were included.
Results
From 2007 to 2016, the rate of twin pregnancies increased (1.37% vs. 1.91%, respectively, P<0.0001). The risk of preterm birth (adjusted odds ratio [aOR], 1.77; 95% confidence interval [CI], 1.66–1.89) also increased; however, the risk of twin growth discordance (aOR, 0.90; 95% CI, 0.82–0.99) decreased. The risks of cesarean section (aOR, 1.16; 95% CI, 1.03–1.29), gestational diabetes mellitus (aOR, 2.10; 95% CI, 1.83–2.39), and postpartum hemorrhage (aOR, 1.27; 95% CI, 1.14–1.41) all increased from 2007 to 2016.
Conclusion
Twin pregnancy outcomes have changed significantly in Korea over a recent 10-year period.
Introduction
Twin pregnancies are well-known for their high risk; it is associated with obstetric complications, such as preterm birth, low birth weight, gestational hypertension, and postpartum hemorrhage (PPH) [1–3]. Over the past few decades, owing to advances in assisted reproductive techniques (ARTs), anthropometry, and increasing maternal age, the twin birth rate has increased worldwide. The twin birth rate in the United States in 2011 was 33.2 per 100 live births, double that in 1975 [4,5]. In Korea, ARTs were introduced in 1986, and the government has provided financial support for infertile couples since 2006 [6]. After the provision of government support, the twin birth rate sharply increased, by 7–10% per year [7]. Despite the increase, data on twin pregnancy outcomes in Korea are lacking.
Much research has been conducted on preterm birth prevention and antenatal steroid use. However, studies on secular trends have focused on singleton pregnancies. However, despite the reported increase in twin preterm birth rate, data on maternal complications and pregnancy outcomes are limited.
Changes in twin delivery and pregnancy outcomes must be monitored to promote maternal health and neonatal care. Hence, the aim of this study was to evaluate the changes in twin pregnancy outcomes between 2007 and 2016 using nationwide Korean population data.
Materials and methods
1. Dataset
This study was conducted using two different datasets. First, data were obtained from Korea’s Vital Birth Statistics for 2007 and 2016. In Korea, birth certificate records are based on records compiled by doctors or nurses at delivery and registered with regional public health centers. The data we collected for this study included birth weight, neonatal sex, parity, multiple pregnancies, gestational age at delivery, and parental age. Gestational age at delivery is usually calculated based on the last menstrual period and is confirmed by ultrasonic examination during the first trimester.
Second, data on pregnancy outcomes in twin-pregnant women were collected from the Korea National Health Insurance (KNHI) Claims Database of the Health Insurance Review and Assessment Service (HIRA) for 2007 and 2016. In Korea, 97% of the population is enrolled in the obligatory KNHI program. Health insurance policies require healthcare providers to allow HIRA to review the medical costs incurred during the treatment of patients. The remaining 3% of the population is covered by the Medical Aid program. Thus, the HIRA database comprises information on all claims for approximately 50 million Koreans, and nearly all information on disease incidence can be obtained from this centralized database.
2. Outcomes
Women with twin pregnancies were identified using Korea’s vital birth statistics dataset. The twin birth rate was defined as the ratio of the number of twin births to the total number of births in the year. Data on birth weight, birth weight discordance, and preterm birth were evaluated. Birth weight discordance was defined as a difference of 20% or more in the weight of the twins, calculated as (larger twin birth weight-smaller twin birth weight)/larger twin birth weight×100. Preterm birth was defined as birth at 37 weeks of gestation or before.
Data on pregnancy outcomes were extracted from the HIRA dataset for women with twin pregnancies between 2007 and 2016. Pregnancy outcomes included gestational diabetes mellitus (GDM), preeclampsia, PPH, placenta previa, and placental abruption, obtained according to International Classification of Diseases, tenth edition codes, and cesarean section, uterine artery embolization, and hysterectomy, obtained using procedure codes.
3. Statistics
Continuous and categorical variables are expressed as means±standard deviations and percentages, respectively. Clinical characteristics were compared between 2007 and 2016 using the t-test for continuous variables and the chi-squared test for categorical variables.
Birth weight according to gestational age was compared between 2007 and 2016 by using a generalized linear model with a compound symmetry covariance structure. Multivariable logistic regression analysis was used to estimate the adjusted odds ratios (aORs) and the 95% confidence intervals (CIs) for the differences in pregnancy outcomes between 2007 and 2016. For multivariable analyses, a fixed set of known risk factors for adverse pregnancy outcomes was adjusted for potential confounding factors, such as maternal age and primiparity. Statistical analyses were performed using SAS for Windows v9.4 (SAS Institute, Inc., Cary, NC, USA).
Results
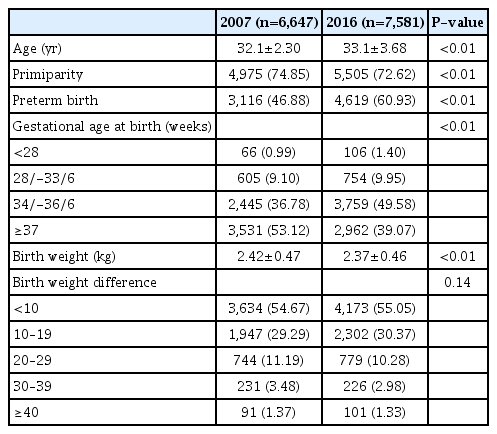
According to Korea’s vital birth statistics, twin pregnancy rates increased from 1.37% (6,647/485,479) in 2007 to 1.91% (7,581/397,445) in 2016 (P<0.01). Table 1 summarizes the basic characteristics of women with twin pregnancies and their pregnancy outcomes in 2007 and 2016. The average maternal age increased while the proportion of primiparity decreased from 2007 to 2016. The preterm birth rate was 60.93% (n=4,619) in 2016, an increase compared with the 46.88% (n=3,116) in 2007.
The pregnancy outcomes in 2007 and 2016
The distribution of gestational age at birth differed between 2007 and 2016. In particular, late preterm births accounted for almost half of twin pregnancies (49.58%) in 2016.
The average birth weights were 2.42 kg and 2.37 kg in 2007 and 2016, respectively (P<0.001). The distribution of birth weight differences did not differ between 2007 and 2016.
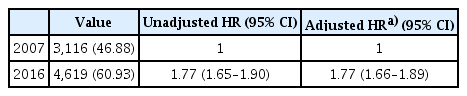
Table 2 summarizes the regression analyses for the risk of preterm birth in twin pregnancies in 2016 compared with that in 2007. After adjustment for maternal age and parity, the risk of preterm birth (aOR, 1.77; 95% CI, 1.66–1.89) increased from 2007 to 2016.
Risk of preterm birth
The birth weight according to gestational age is illustrated in Fig. 1. In the generalized linear model with a compound symmetry covariance structure, after adjustment for maternal age, parity, and neonatal sex, no significant difference in birth weight according to gestational age was observed between the two periods.
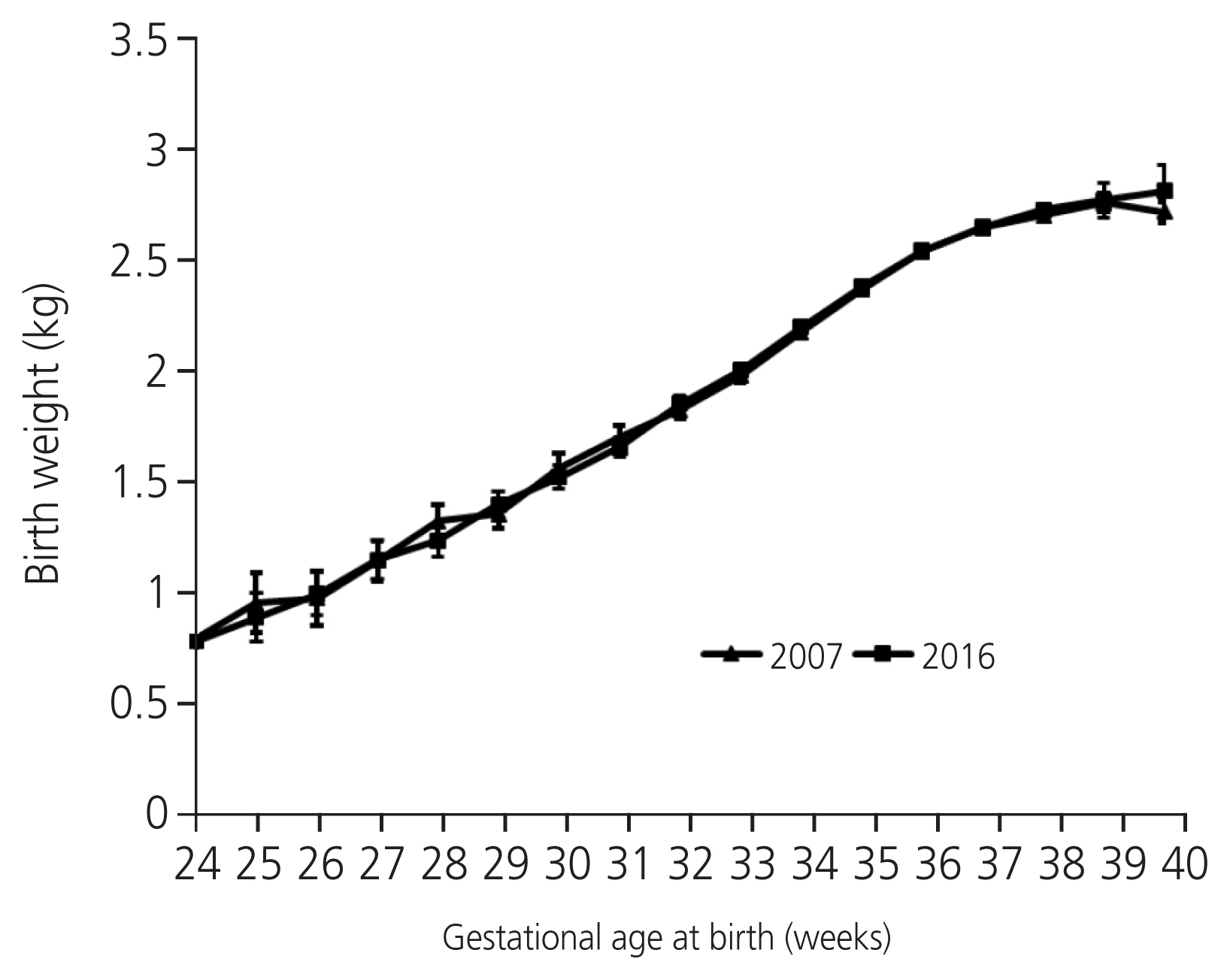
Birth weight according to gestational age at birth.
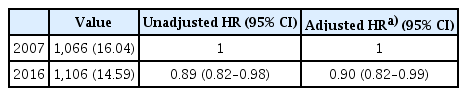
Table 3 summarizes the regression analyses for the risk of birth weight discordance; the risk decreased from 2007 to 2016 after adjustment for maternal age and parity (aOR, 0.90; 95% CI, 0.82–0.99).
Risk of birth weight discordance
Pregnancy outcomes were evaluated using the HIRA database. Fig. 2 displays the pregnancy outcomes in each group. The risk of cesarean section, GDM, and PPH increased from 2007 to 2016 after adjustment for maternal age and parity; however, the risk of hysterectomy decreased.
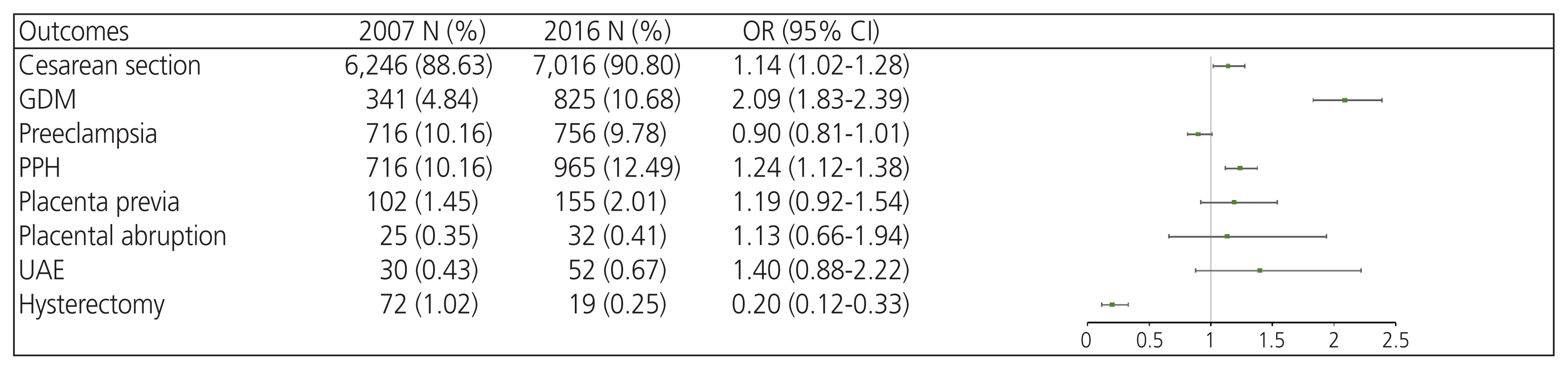
Pregnancy outcomes between 2007 and 2016. OR, odds ratio; CI, confidence interval; GDM, gestational diabetes mellitus; PPH, postpartum hemorrhage; UAE, uterine artery embolization.
Discussion
In this study, we revealed an increase in the twin birth and twin preterm birth rates during the study period. In particular, late preterm births accounted for a large proportion of premature twin births. However, other neonatal prognostic factors, such as birth weight discordance and weight according to gestational age, did not significantly change.
The increase of ART use in Korea is probably one of the main reasons for the rise in twin births during the study period. The HIRA has been supporting infertile and subfertile couples, in terms of providing appropriate treatment, since 2006. In 2015, the Ministry of Health and Welfare introduced guidelines on ARTs, restricting the number of transferred embryos to three, citing the increased ART-related complications. During the study period, two or more embryos were transplanted in more than half of the patients. As a result, two or more gestational sacs were identified in 21.4% of pregnant women in 2017. The ratio of dizygotic to monozygotic twins also went up from 2.4 in 2006 to 2.97 in 2017 [7–9].
The increase in preterm births in twin pregnancies can be explained by various factors other than maternal age and parity. First, lifestyle factors, such as occupation and obesity, may have increased the preterm births in twin pregnancies, similar to the case with singleton pregnancies [10]. The increase in ART use may also have been responsible, for instance owing to ART-related complications, such as placenta previa and embryo reduction [11]. Finally, as accessibility to hospitals has improved, iatrogenic factors may have caused more preterm births. This possibility is supported by the larger proportion of late preterm births among the prematurity population and the lower proportion of twins with birth weight discordance. In addition, in the case of twins, unlike that of singletons, the delivery time is determined according to chorionicity and amnionicity [12,13]. The American College of Obstetricians and Gynecologists suggested that obstetricians consider delivering twins in the preterm to early term according to their chorionicity. Early obstetrical intervention and medically indicated preterm delivery may thus have resulted in the increase in twin preterm deliveries.
The overall increase in the preterm rate may play an important role in the increase in twin preterm deliveries. Late pre-term birth has a better prognosis than birth before 34 weeks. However, preterm-associated morbidity is reportedly higher than that observed in full-term singleton neonates [14–16]. In this context, the appropriate timing of delivery and steroid use in multiple pregnancies needs to be investigated to enable better systematic perinatal care for multiple pregnancies. However, owing to the limitations of the study design, indications for delivery and chorionicity are lacking. Further studies are needed to demonstrate causal relationships in this regard.
We also evaluated changes in pregnancy complications during this period. The risk of GDM increased approximately two-fold from 2006 to 2017 after adjusting for maternal age and parity. GDM is on the rise owing to changes in maternal lifestyle and obesity rates [17,18]. It is a well-known fact that preeclampsia and GDM share common risk factors. In a previous study, the prevalence of preeclampsia in the overall population and among women with singleton pregnancies increased substantially from 2001 to 2014 in Taiwan [19]. However, the relative risk of preeclampsia did not increase from 2007 to 2014. Laine et al. [20] discovered, in a largescale epidemiological study in 2019, that twin pregnancies are the largest risk factor for preeclampsia, yielding a fourfold increase in the risk, even after adjustment for other risk factors. Therefore, we infer that preeclampsia in twins is influenced by genetic effects, abnormal placentation, and twinning itself rather than environmental effects.
The rate of cesarean sections increased in twin pregnancies from 88.6% in 2007 to 90.9% in 2016, as well as in total births over the same time period. Cesarean section is widely accepted as an appropriate method for twin delivery [21]. The relatively higher risk of failure in vaginal delivery compared with singleton births, the mothers’ preference for cesarean section and dislike towards prolonged labor, and legal issues may all have influenced obstetricians to choose cesarean section over vaginal delivery [22].
Twin pregnancy is a leading risk factor for PPH. During this study period, the incidence of PPH increased 1.3-fold; however, the incidence of hysterectomy significantly decreased. This may be related to the advances in and widespread use of embolization techniques.
As this was a retrospective study, in the results should be interpreted with caution, as the indications for delivery were not specified. In addition, information on chorionicity and the ART rate, which are factors that determine prognosis in twins, was limited. Nevertheless, this study provides important data regarding twin pregnancy outcomes among Koreans. This study was more comprehensive than previous studies, as it included other pregnancy complications, providing additional considerations in the management of twin pregnancies.
In conclusion, twin pregnancy outcomes have changed significantly in Korea over a recent 10-year period. These results should be considered when women with twin pregnancies are counseled.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Ethical approval
This study was approved by the Institutional Review Board (IRB) of the Korea University Guro Hospital (2021GR0398).
Patient consent
This study was exempt from review and the requirement for informed consent was waived by the IRB.
Funding information
None.