Social determinants of mental health of women living in slum: a systematic review
Article information

Abstract
Objective
With the rise of urbanization globally, the problem of living in slums has become a problem for the civil society. As a vulnerable segment, women make up half of the population in these regions; therefore, women’s mental health has always been a concern. The purpose of this study was to review the social determinants of mental health in women living in slum areas.
Methods
We systematically reviewed articles published between 2009 and 2019 on the social determinants of women’s mental health in SID, Magiran, Google scholar, PubMed, Scopus, Science Direct, Embase, MEDLINE, PsychINFO, and PsychARTICLES databases using MeSH keywords according to PRISMA guidelines. The quality of the studies was assessed depending on the type of study using Ottawa Newcastle” scale and Joanna Briggs Institute quality assessment tools. Finally, 23 studies were analyzed.
Results
Different social determinants influenced the mental health of women living in slum areas. Among the structural determinants, the socioeconomic level had the highest frequency, and gender was in the second rank with the highest correlation with poorer women’s mental health status. Among the intermediate determinants, living conditions, food insecurity, social capital, and social support were most frequently associated with mental health status.
Conclusion
Women living in slum areas are prone to developing mental disorders and poorer mental health; therefore, supporting these women and creating job opportunities to raise their incomes and, subsequently, improve their social, economic, and living conditions should be taken into consideration. In addition, this requires careful planning and comprehensive social support.
Introduction
In recent years, owing to the expansion of urbanization, residents have been given the opportunity to access extensive health care facilities [1].
However, this expansion has led to more number of residents living in slums, especially around large cities [2]. With the unexpected growth of urbanization, living in slums has become a pervasive problem in many parts of the world, causing many social consequences [3].
Residents living in slums are prone to diseases, injuries, premature death more than those not residing in slums; moreover, the disease, coupled with poverty and its harmful effects, increases over time [4,5].
In the World Health Organization (WHO) Statute, drafted in 1946, health is defined as “the state of complete physical, mental, and social well-being and not merely the absence of disease” [6]. Health is, individually and socially, one of the most important aspects of human life. Health is a prerequisite for social roles; therefore, all human beings can be fully active in society if they are healthy. Health has many dimensions, one of which is mental health [7].
Mental health is an aspect of the general concept of health and is defined as the power to live calmly with oneself and others; moreover, it also involves to be calm, aware of oneself and one’s feelings, make decisions in times of crisis, and successfully cope with stress [8]. Mental health is an art that helps people to psychologically and emotionally adapt to their environment and to choose the most desirable solutions to solve their problems, as people cannot be effective in carrying out their social responsibilities if they are mentally burdened. Today, mental health is very much in focus [9,10].
Social determinants of health are the conditions in which people are born, grow, live, and work. Justice in health means the absence of preventable health differences among populations or groups of society that can be caused by differences in racial, economic, demographic, or geographical status. Health, which a community can achieve using methods that lead to interdisciplinary participation and collaboration, is a multifaceted subject; therefore, a look at the social determinants of health shows that the provision, maintenance, and promotion of a community’s health is not realized solely by the Ministry of Health [11].
Systematic reviews summarize the reported results with clear goals and provide the best evidence for judgment [12,13]. Women constitute half of the population of any society, and they play diverse social and economic roles. Women’s health is at the core of ensuring the functioning of families and communities and is of particular importance in providing and maintaining family and community health. Given the special conditions of living in suburban areas and the importance of mental health of women as a vulnerable group, we aimed to systematically review factors affecting the mental health of women living in slums.
Criteria for considering studies for this review
1. Search strategy
This study was reported based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [14]. Web of Science, MEDLINE, SID, Magiran, Iran doc, Google Scholar, PubMed, Scopus, Science Direct, Embase, MEDLINE, PsychINFO, PsychARTICLES databases were searched for articles published between 2009 and 2019. Keywords were selected using the MeSH keyboard (Table 1).

Search strategy
According to the WHO model, social determinants of health are socioeconomic structural factors such as income, education, employment, social class, gender, race, and ethnicity; intermediate factors such as living conditions; behavioral and biological factors such as physical activity, alcohol consumption, and tobacco use; and health system-related factors [15].
2. Inclusion and exclusion criteria
Studies published in Persian and English between 2009 and 2019 that examined factors affecting the mental health of women living in suburban and slum areas with different ages and income levels were included.
Articles with no access to full-text articles, articles written in languages other than English and Persian, study protocols, case studies, brief reports, and studies conducted on women with known psychological problems requiring treatment were excluded.
3. Study selection
An initial search yielded 1,743 results. The eligibility of these papers was independently evaluated by 2 authors, and any disagreements were resolved by consensus. In the first stage, 1,007 papers were excluded because they were irrelevant or duplicated. After reviewing the titles and abstracts of the remaining papers, 300 more papers were excluded. During evaluation of full texts, 200 out of the remaining 436 articles were excluded owing to being ineligible. Finally, a total of 23 eligible articles were reviewed (Fig. 1).
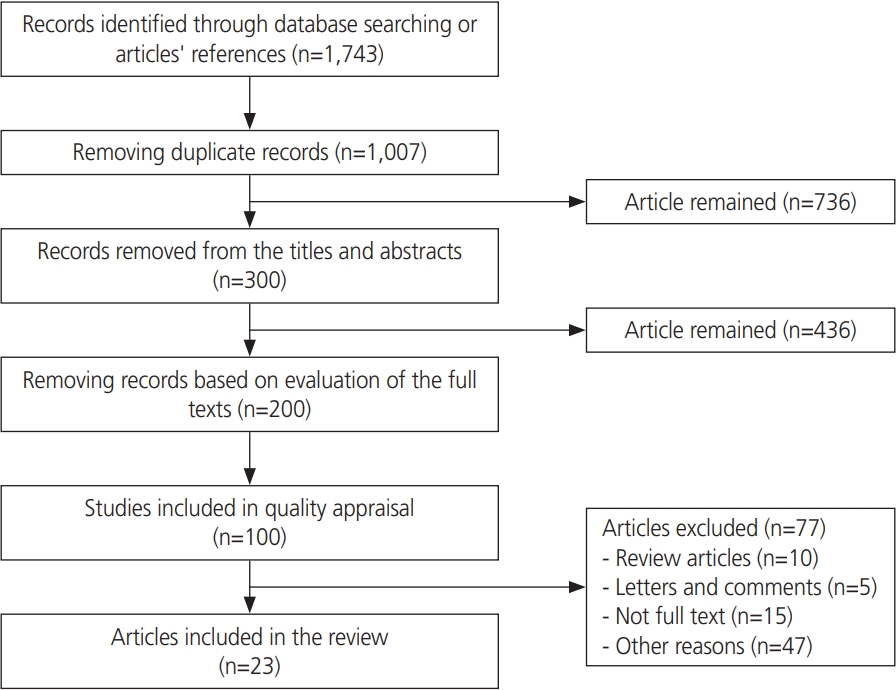
Search flow diagram.
4. Quality assessment
The Newcastle–Ottawa scale (NOS) was used to assess the quality of the studies. This scale is used to measure the quality of cohort and case–control studies. The validity and reliability of this tool have been proven in various studies (Table 2). The checklist items focused on reporting or evaluating different sections of observational studies. Qualitative studies were assessed using the Joanna Briggs Institute (JBI) checklist (Table 3) [14,39].
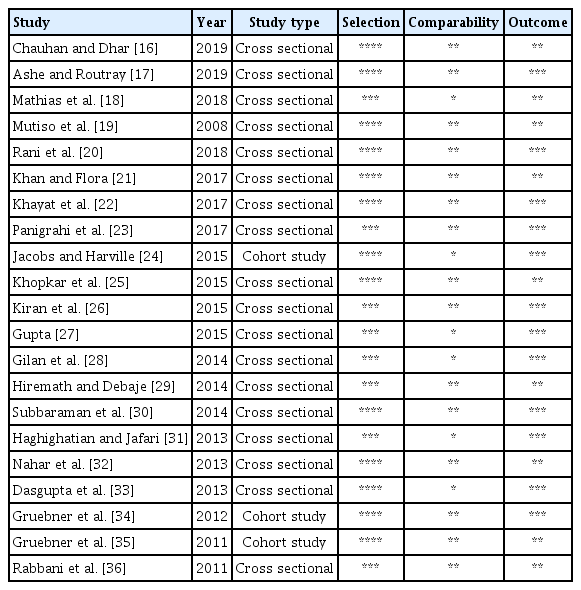
Quality assessment of the studies by “Ottawa Newcastle” scale

Qualitative studies assessed by Joanna Briggs Institute (JBI) checklist
5. Data extraction
Two authors independently performed the study selection and validity assessment and resolved any disagreements by consulting a third researcher. Data on first author name, publication year, study design, sample size, geographic region, age, social determinants of mental health, tools, results, and quality assessment were extracted and entered for analysis.
Results
After evaluating and determining the final quality of articles, 23 relevant articles were selected (Table 1). As observed, most of the articles had a quantitative design (n=20). Other studies had a qualitative (n=2) and mixed method (n=1) design. A total of 6,755 women were examined in different age groups such as adolescence, middle age, reproductive age, and older age (total age range, 10–81 years). Studies were conducted on women from the suburbs and slums of numerous countries. The largest number of studies were conducted in India (n=12), followed by Bangladesh (n=4), Iran (n=4), Kenya (n=1), Mexico (n=1), and Nepal (n=1).
1. Structural factors
As shown in Table 4, different social determinants can contribute in improving or weakening women’s mental health. The reviewed studies examined different aspects. Structural factors such as gender, level of education, age, social and economic status, household income, marital status, number of households, place of birth, occupation, religion, and place of residence were among the factors covered [16-19,21,23-28,30-32,34,36-38]. The strongest factors that could affect mental health according to the studies were related to household income and socioeconomic status, which were highlighted in 10 studies [16,17,21,23,26,30,34,35,37,38]. These studies indicated low income, poverty, and low socioeconomic status can lead to poor mental health in women. The second factor affecting women’s lower mental health was gender. Seven articles examined the relationship between gender and mental health [16,17,19,25,27,30,34], three of which showed that women were more susceptible to mental disorders [16,17,30], one study reported this issue in men [25], and three studies showed no relationship in this regard [19,27,34]. Six studies also examined the relationship between age and mental health [21,24,26-28,34]. Five studies showed increasing age and age at birth of the first child [21,24,26,28,34], and one study did not show any association [27]. Job status was examined in 5 studies [26,28,34,36,38] that showed that unemployment, being a housewife, and dissatisfaction were related to a low level of mental health. Another factor was living in the suburbs and slums [19,30,32]. Three studies showed that living in the slums is one of the factors that affect women’s mental health, which is aggravated by overcrowding in these areas. A low level of education of women themselves or their parents at adolescence can potentially cause poor mental health in these areas [16,21,25,36]. Marital status was also examined in 3 studies, which concluded that married women had poorer mental health than unmarried women [16,26,36]. The number of family members can also have an impact on mental health, with women with more children and a busy family having a poorer mental health than women with a smaller family [28,34].

Results from a systematic review of studies
2. Intermediate factors
Disease status [17,28,30] and disability [30] were studied in four articles. Chronic diseases such as diabetes and hypertension or physical disabilities can also be linked to mental disorders in women.
Social determinants of mediators affecting mental health may also include living conditions [27,34,35], family conditions [17,23,34,37], domestic violence [22,29,33], nutritional status [20,21,25,34,35], and social factors [18,23,31,35,38].
Four studies found that inadequate living conditions, such as poor ventilation, poor cooking conditions, social living conditions, and living away from green spaces could be associated with poor mental health.
Abuse by spouse following alcohol consumption [33], family members’ addiction [23], death of family members, family members’ illness [17], lack of understanding by family members [23], and family disputes [17] are among the factors influencing women’s mental health. Family members’ illness comprised the largest proportion and was discussed in 2 articles [17,38].
The likelihood of natural hazards such as flooding was assessed in 3 studies, and a direct relationship was shown between the risk of natural disasters and poor mental health [24,35].
Domestic violence, such as sexual and physical violence, was reported in 3 studies [22,29,33], and its relationship with the incidence of mental disorders in women has been demonstrated.
Nutritional status was assessed in 5 studies [20,21,25,34,35]. The lack of food security in the family was reported in 2 studies, and another study found that a poor nutritional status of mothers effectively lowered the level of women’s mental health. The same was true for obesity and overweight.
Social factors [18,23,31,35,38] such as the lack of social trust, social cohesion, social norms, social capital; low social support from the community, family, friends and co-workers; poor social fabric; low security; and negligence with respect to social norms can also be associated with poor mental health in women.
According to the Nae Disha curriculum [18], strengthening and training areas; building emotional competence and peer relationships; and strengthening social networks, self-belief, and resilience tones are effective in promoting the mental health of slum women.
Other factors associated with low levels of women’s mental health include caste, media exposure [16], child wasting, child underweight [21], pallor, low physical activity, and obesity [26].
The tools used to screen for mental health and other factors are also listed separately in each study. As observed, the General Health Questionnaire (GHQ) was used in 5 studies with the highest frequency. Its 12-item form was used in 3 studies, and its 28-item form was used in 2 studies. Two studies also used the WHO-5 questionnaire for mental health screening.
Discussion
In the present study, the findings indicate that social health determinants affect slum women’s mental health. Among the structural determinants, gender and social class (education, job, and socioeconomic status) correlated the most. According to the results, the higher the socioeconomic status and income level of this segment of society, the worse the mental health status of women. Recent findings are in line with the results of Weinberg et al. [40]. They found, in a 16- year study in the Netherlands, that socioeconomic status and educational attainment inversely and negatively correlated with mental health in adults. Sweeney et al. [41] found that socioeconomic deprivation was associated with an adverse public health status. The use of mental health services in this group of people is different from that of other groups, and they have less access to medical services to manage their mental health problems. In this group, there are more unemployment disorders that increase social stigma, which can lead to undesirable consequences such as social isolation, inappropriate health behaviors, and an exacerbation of mental problems [41].
Influential social factors reflect different positions of people in the social ladder of power and resources. Evidence suggests that most illnesses and health inequalities in the world stem from social factors. The context of these factors shows that in many countries, it is impossible to achieve health goals without achieving significant success in poverty alleviation, food security, education, women’s empowerment, and improved living conditions in poor and densely populated areas. The definitive role of social and environmental factors that affect people’s health has long been recognized. Epidemiological research has proven that environmental and social factors have been important in improving the health of many populations in industrialized countries at the turn of the century. The WHO Statute, drafted in 1946, addressed the fact that its founders intended to address the social roots of health problems as well as confront the challenges of effective health care and treatments. In this statute, health is defined as “the state of complete physical, mental, and social well-being and not merely the absence of disease” [6].
Education is one of the determinants of social class and socioeconomic status [4]. In the modern world, education is seen as a means of improving the quality of life of individuals and has a strong effect on mental health; moreover, studies suggest that there is a significant positive relationship between low education and mental disorders such as severe depression [21]. Carter et al. [42] also found that class discrimination directly and significantly correlated with education levels, depressive symptoms, and anxiety, and these results are consistent with findings from a recent study. Studies conducted in Iran also indicated that the education of slum women is low, such that in a cash study by Naghdi and Zare [43], 86.7% of women living in slums in Shiraz were illiterate or had elementary or secondary education. Similar results were also found in studies conducted in other countries. Of women living in slums, 12.8% were mostly illiterate and 80.6% had primary and secondary education [44]. Generally, illiteracy and low literacy in the slums and suburban areas is a significant problem associated with socioeconomic status and mental health.
Gender was another factor that was most frequently reported in the studies related to mental health. According to the findings of the studies, women were more susceptible to mental disorders than men. This finding is consistent with that of Gitay et al. [45]. In their study of 300 students in Pakistan, they found that women experience mental disorders such as anxiety and depression more than men [45]. Among the intermediate determinants, living conditions, food insecurity, social capital, and social support were most frequently associated with mental health. Living conditions and lifestyle are intermediate health determinants that can be directly or indirectly related to people’s health [46]. According to current findings, various aspects of adverse living conditions such as inadequate housing, social living conditions, and being away from appropriate living facilities are associated with the mental health of this vulnerable group. Khayat et al. [46] in their study of slum women in Zahedan found that women in these areas were experiencing very poor living conditions and health status, which resulted in a lower public health status than other women living in the same city. In addition, because of their living conditions, slum women are exposed to various kinds of violence and stress that have a negative relationship with their mental health status [47].
Food insecurity is another intermediate determinant of health that is linked to the health of people based on the WHO model. The results of various studies show that low income is clearly an important determinant of food insecurity, although other factors such as limited access to food assistance programs, low education, and the number of family members are also associated with increased food insecurity. In a study by Yadegari et al. [48], they found that food insecurity through stress, body mass index, and depression affects pregnancy outcomes, and this is consistent with the results of the reviewed studies. Social support and social capital are other intermediate determinants associated with mental health. According to the results of the studies, the more inappropriate supportive roles these people had, the more difficulties and mental disorders they experienced. According to a model presented by Nieminen et al. [49] on the relationship between social capital and social support with mental health, these 2 factors directly and indirectly influence the mental health of patients. As discussed, social determinants of health, owing to their importance and role, are increasingly being identified as factors influencing individuals’ physical and mental health, and these health predictors require more attention.
In conclusion, structural determinants, i.e., gender and social class (education, job, income, and socioeconomic status) were most frequently associated with mental health. Among the intermediate determinants, living conditions, food insecurity, social capital, and social support were most frequently associated with mental health. The mental health of women, who constitute half of the suburban community and the foundation of families, should be considered as the highest level of health. Extensive social support and planning for the employment of women and their family members as well as helping improve their income and enhancing their socioeconomic status can improve their mental health, as women in these areas are more prone to having poor mental health. Improving the socioeconomic status ensures food security for women, thus improving their nutritional status.
Limitations of this study include women’s unwillingness to participate in women’s studies, self-reporting and information recall by women, the use of a tool for mental health screening in studies, the greater likelihood of slum women residing in an area to participate in the study, the lack of representativeness, and the lack of access to full texts of a few articles.
Acknowledgements
We also appreciated Alborz University of Medical Sciences.
Notes
Conflict of interest
No potential conflicts of interest relevant to this article were reported.
Ethical approval
This study was approved by the Alborz University of Medical Sciences with ethnical code IR.ABZUMS.REC.1398.161.
Patient consent
None.
Funding information
None.