Delayed intestinal perforation and vertebral osteomyelitis after high-intensity focused ultrasound treatment for uterine leiomyoma
Article information

Abstract
High-intensity focused ultrasound (HIFU) is a non-invasive uterine fibroid treatment option for patients who want to preserve fertility. However, according to several reports regarding ablation of solid tumors by HIFU, there are rare complications in patients with uterine leiomyomas, and overall data are still insufficient. Here, we report rare and major complications of HIFU, such as delayed intestinal perforation, uterine perforation with recto-uterine fistula, and osteomyelitis 29 days after the HIFU procedure to treat multiple myomas. Thus, we present a very serious case resulting from HIFU treatment of uterine fibroids and a review of the literature.
Introduction
High-intensity focused ultrasound (HIFU) has a role in ablating tumors by changing the frequency, which is unlike that of diagnostic ultrasound [1]. For decades, HIFU has been used to treat solid tumors such as prostate [2], liver [3], and breast [4]. Because it is minimally invasive, HIFU has recently been spotlighted for the treatment of uterine fibroid tissue [56]. Theoretically, HIFU procedures for removing fibroid tissue are preferred over a hysterectomy in unmarried and nulliparous women who want to retain their ability to bear children. Further, there are fewer hospital days and days without usual activities resulting from HIFU procedures than those experienced after surgical procedures. However, complications such as skin burns, fever, and low abdominal pain can occur in mild cases, and complications such as intestinal perforation and uterine bleeding can occur in severe cases [7]. We experienced a case of delayed intestinal perforation, uterine perforation with recto-uterine fistula, and vertebral osteomyelitis after HIFU procedure for treating multiple myomas, which is reported here to document potential side effects of HIFU.
Case report
A 43-year-old gravida 1, para 1, married women who presented with abdominal pain and abdominal distension was referred to our institution for treatment in January 2016. She had received HIFU ablation for multiple leiomyoma 29 days earlier. She was diagnosed with hypothyroidism in 1998. Her previous operative histories were abdominal surgeries for myomectomy in 2003 and appendectomy in 2012. She also had a cesarean section for delivery of a twin pregnancy in 2015. In December 2015, she underwent HIFU ablation with a HIFUNIT 9000 tumor therapy system (Shanghai Aishen Technology, Shanghai, China) to remove 6 uterine intramural leiomyomas approximately 3 cm in size and causing menorrhagia and abdominal discomfort. Immediately after the HIFU procedure, she had abdominal discomfort and distension; however, the pain subsided after administration of a non-steroidal anti-inflammatory drug. Fourteen days after the procedure, the abdominal pain was aggravated and she developed pain when defecating. She was admitted to a local hospital 29 days after the procedure, attributable to the aggravated symptoms. Her symptoms were not relieved, and she was transferred to our hospital for further evaluation. Her blood pressure was 122/65 mmHg, pulse rate was 112 beats per minute, breathing rate was 20 breaths per minute, and body temperature was 37.6℃. She appeared to be acutely ill, with redness and swelling in her periumbilical area, as well as tenderness and rebound tenderness in a distended abdomen. During a pelvic exam, vaginal bleeding was not observed; however, a brownish-colored vaginal discharge was found with a foul odor. Initial hemoglobin level was 9.4 g/dL, white blood cell count was 5,560/µL, and platelet count was 193,000/µL. The prothrombin time was prolonged to 20.8 seconds (reference: 11.8–14.3 seconds). Fibrinogen level was elevated to 500 mg/dL (reference: 180–400 mg/dL), and serum C-reactive protein level was also elevated to 28.4 mg/dL (reference: <0.5 mg/dL). A transvaginal ultrasound showed hyperechoic calcification lesions and 0.4-cm sized fluid collection around the uterus (Fig. 1). In abdomen-pelvic computed tomography (CT), there were several air-density lesions observed in the whole abdomen and air-fluid levels were noted in the anterior abdominal wall (Fig. 1). Additionally, air-density was found at the T5 and S1 vertebra level (Fig. 1). The anterior and posterior walls of the uterus were destroyed, accompanied by panperitonitis and pneumoperitoneum. Therefore, we performed an emergency operation for panperitonitis and rupture of uterus.
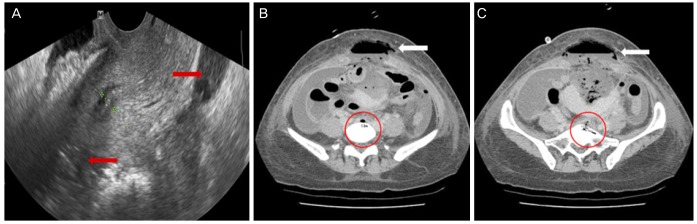
(A) Transvaginal sonography: fluid collection around uterus (red arrow). (B, C) Air-fluid level of anterior abdominal wall (white arrow) in abdomen-pelvic computed tomography (CT): air-density of L5 (B) and S1 (C) level of vertebra (red-circle).
During surgery, necrotic changes were found in the rectus muscle, fascia, peritoneum, and omentum of the abdomen below the level of umbilicus. When the abdomen was opened, there was fluid collecting with a foul odor from the subcutaneous area to the retroperitoneal wall. Necrotized and perforated uterine walls were located. Adhesions among the posterior wall of the uterus and left adnexa and intestine were noted with necrotic changes. After adhesiolysis, a 1.5-cm perforation of the colon was found approximately 10 cm above the anal verge abutting the retroperitoneum to left lateral side (Fig. 2). Further, we found necrotic changes in the retroperitoneal wall. After removing the debris, a subtotal abdominal hysterectomy with left salpingo-oophorectomy and transverse end loop colostomy were performed (Fig. 2).
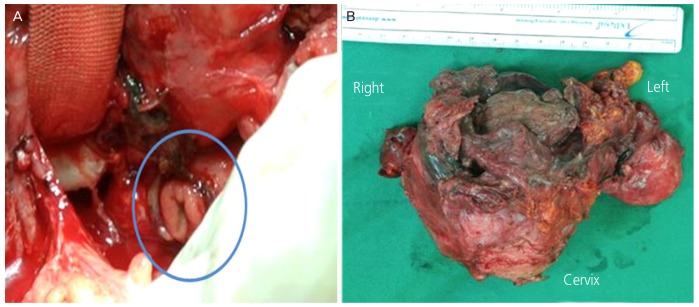
(A) 1.5-cm sized perforation of the colon (blue circle) was found approximately 10 cm above the anal verge. (B) Subtotal abdominal hysterectomy and left salpingo-oophorectomy.
Vital signs and symptoms of the patient were stable after surgery and she was discharged 23 days post operation. Three weeks after discharge, she noted pain in her back. Bone destruction at the L5 vertebrae level with loculated fluid collection in the pelvic cavity was shown by magnetic resonance image of the lumbosacral spine lesion. It was presumed that direct invasion of the abscess was the cause of vertebra osteomyelitis, and the patient was again admitted to orthopedics. A CT-guided biopsy of the osteolytic lesion was performed, showing acute inflammatory cell infiltration in the marrow and a few small necrotic bone fragments. CT-guided aspiration cultures from the pelvic cavity did not isolate a pathogen; however, cultures from the cervix grew Escherichia coli and Enterococcus faecalis. After treatment with antibiotics (ceftriaxone [Ceftriaxone®; Aju Pharmaceutical Co., Seoul, Korea] and metronidazole [Flagyl®; JW Life Science, Seoul , Korea] for 1 week and then ampicillin/sulbactam [Unasyn®; Pfizer Inc., New York, NY, USA] and ciprofloxacin [Cycin®; Ildong Pharmaceutical Co., Seoul, Korea] for 3 weeks), the symptoms were relieved and the patient was discharged.
Discussion
HIFU can be used to ablate targeted uterine fibroids locally without surgery such as a myomectomy or hysterectomy [1]. In addition, patients who are treated for uterine fibroids by HIFU do not experience surgical complications and do not require additional surgeries. The occurrence of complications such as pain, fever, and infection accompanied by surgery is lower in HIFU patients than in surgery patients [8]. It has been reported that severe complications, such as rectal wall injury and recto-urethral fistula can occur after a HIFU procedure [1]; however, these severe complications are thought to rarely occur, attributable to improvements in device design and technology [9]. Ren et al. [10] reported that approximately 19% of all patients treated with the HIFU procedure experience mild symptoms that last for approximately 1 week. Chen et al. [7] reported that severe complications such as skin burns, acute renal insufficiency, and intestinal perforation may occur. According to this report, approximately 0.06% of all patients experience these complications and require additional major therapy and prolonged hospitalization. In the report by Chen et al. [7], there were 2 cases of intestinal perforation out of 1,305 complications, and in these cases, perforations were found 10 days and 12 days after each procedure. In the case presented here, intestinal perforation was detected 29 days after the HIFU procedure, and more time was required to diagnose the bowel complication in comparison to other cases.
There are no reports about osteomyelitis after the HIFU procedure. Thus, to the best of our knowledge this is the first report regarding HIFU complications in association with osteomyelitis, an inflammatory state of the bone caused by a microorganism. One disease mechanism is local spreading from a contiguous focus of infection, and several bacteria and fungi are common infecting microorganisms [11]. Contiguous infection is most commonly seen with direct contamination of bacteria in open fractures of joint replacement surgery with an orthopedic implant. Rarely, an unusual source of contamination is reported from a gunshot wound to the abdomen [12]. We found necrotic changes in the retroperitoneal wall during surgery; therefore, our case provided a contamination source to the lumbar and sacrum spines. Thus, once diagnosed, antibiotic therapy was the first choice of treatment [13].
HIFU is a treatment option for patients who want to preserve fertility and a non-invasive procedure for treating uterine fibroids. However, as in the above case, we must consider that HIFU can cause several serious complications and severely effect patient quality of life. Further, these severe complications are often found 10–29 days after the procedure rather than immediately. Consequently, it is important for clinicians to keep in mind the possibility of these serious complications and observe the patients long term to detect complications. In the future, research should be conducted regarding the advantages and disadvantages of the HIFU procedure, and it should be considered that such complications may result.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.