



Introduction
Intracranial arachnoid cysts are accumulations of cerebrospinal fluid (CSF) between the dura and the brain substance. In contrast to normal arachnoid membranes, arachnoid cysts contain a thick layer of collagen and hyperplastic arachnoid cells in the cyst wall, but fewer trabecular processes within the cyst [1]. These cysts can be classified as either primary or secondary, depending on the absence or presence of prior pathological causes, such as hemorrhage, trauma, and infection [2,3].
Pathogenesis
Although several hypotheses have been proposed to explain the origin of cysts, arachnoid cysts are assumed to result from aberrant subarachnoid development. After 45 days of pregnancy, the arachnoid mater is hydric dissected by CSF and separated from the pia mater, creating the subarachnoid space. However, owing to incomplete separation between the arachnoid and pia mater, a chamber in which CSF collects is formed this time, according to the first theory of arachnoid cyst formation [9,10]. Similarly, the second theory postulates abnormal development of the meninx primitiva as the main mechanism of arachnoid cyst formation. Owing to a defect in mesenchyme condensation, cavitation develops inside the meninx primitiva, which later evolves into arachnoid cysts [11]. Another theory states that a defect in brain genesis generates arachnoid cysts [2]. According to this theory, an empty space is created by primary agenesis and involution of the brain, and this space is secondarily filled with CSF. However, in recent years, these theories are not considered, except in cases of hypoplasia of the temporal lobe or arachnoid cyst with agenesis of the corpus callosum.
Furthermore, several mechanisms could explain the enlargement of these cysts: the unidirectional valve between the cyst and the subarachnoid space, the osmotic pressure gradient between cystic content and CSF, or the production of fluid by the cells that surround the wall of the cysts [12]. Consequently, abnormal meningeal development and unidirectional valve phenomena are the most accepted hypotheses that explain the formation and expansion of arachnoid cysts.
Prevalence and cyst location
The prevalence of arachnoid cysts is approximately 1% in the general population, accounting for 10% of intracranial space-occupying lesions [3,13]. The prevalence in the pediatric population is approximately 1.3-2.6% in studies that reviewed arachnoid cysts detected incidentally on brain magnetic resonance imaging (MRI) [14,15]. In the fetal period, the prevalence of arachnoid cysts was reported to be approximately 0.2-0.9% in studies based on ultrasound scans [8,16] and 1.1% in studies based on MRI [17]. The most common location where these cysts are found in the fetal period is the interhemispheric space in the supratentorial area [16,18], whereas it is the middle cranial fossa in children [14,15]. Thus, the difference in the prevalence and cyst location between the prenatal and postnatal periods can be explained using the diagnostic tools and the pathogenesis of cyst formation. The subarachnoid space of the temporal pole generally regresses during the late fetal period and the first few months of life; however, impeding this process leads to cyst formation. In addition, hemispheric cysts are not often found in children, and it has been hypothesized that they regress spontaneously after birth. The differences in the prevalence and location of cysts between the fetal and childhood periods are shown in Table 1.
Ultrasound or MRI findings of arachnoid cysts
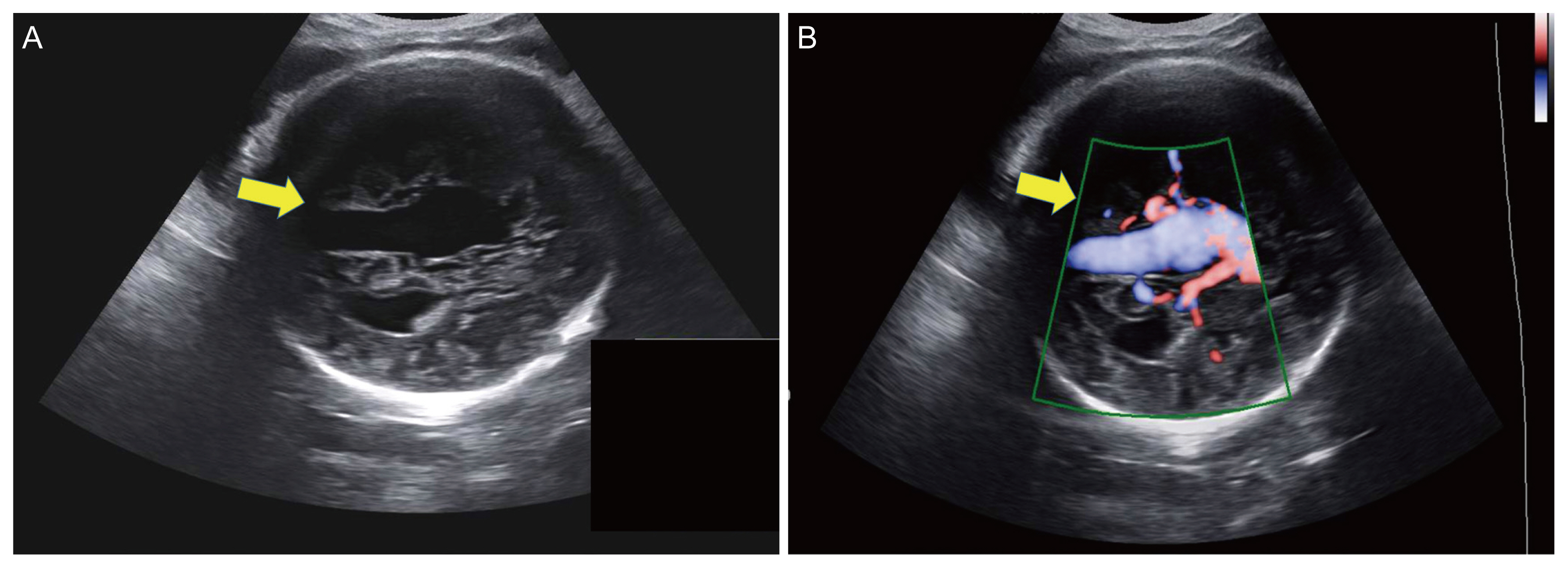
The first detection of fetal intracranial cysts always comes from routine prenatal ultrasonography. On ultrasound, fetal arachnoid cysts appear as well-defined anechoic lesions with no blood flow on color doppler imaging (Fig. 1) [19]. Arachnoid cysts may exist as extra-axial lesions in any location within the brain, in both the supratentorial and infratentorial compartments. One-third of these cysts can compress the brain parenchyma [4,17]. Fetal arachnoid cysts are generally detected after the second trimester of pregnancy, with half of them detected in the second trimester and the other half in the third trimester [8,19]. According to previous studies, fetuses diagnosed with arachnoid cysts after 30 weeks of pregnancy had normal ultrasound findings at 22 weeks of gestation [19]. The mean gestational age at which cysts were detected was 28 weeks [4,8]. Thus, it can be assumed that most cysts were incidentally detected on routine obstetric ultrasound.
Fetal MRI can be performed to assess the extent of complicated congenital diseases [20]. It has been reported that fetal MRI may provide additional information about brain parenchymal lesions, midline structures, posterior fossa anomalies, and malformations of cortical development [21,22]. Although the rate of central nervous system (CNS) anomalies detected exclusively on MRI is lower than that previously reported because of the development of neurosonography, MRI in the third trimester is considered to have a better detection rate for cortical, white matter, and intracranial hemorrhagic anomalies [22]. In addition, several recent studies have reported that fetal MRI is functional in predicting postnatal neurodevelopmental outcomes [23,24]. Moreover, fetal MRI can help clarify the diagnosis of cysts and detect additional abnormalities independent of fetal position and maternal obesity [4,8,19,25].
Since ultrasonography is the first modality for screening for fetal abnormalities, the diagnosis can be changed after MRI. Yin et al. [8] performed MRI on 40 patients with arachnoid cysts on ultrasonography, and five of the patients were diagnosed with other brain abnormalities, such as black pouch cysts, ependymal cysts, and dural sinus malformation. On the other hand, De Keersmaecker et al. [4] reported one patient with ventriculomegaly on ultrasound, whose diagnosis was changed to arachnoid cyst after MRI. Recently, the Korean Society of Ultrasound in Obstetrics and Gynecology Research group reported that the accuracy of ultrasound for diagnosing arachnoid cysts was 72% (unpublished data).
Prenatal diagnosis is strongly recommended because an accurate diagnosis can be made and the prognosis predicted through additional information obtained by MRI. Furthermore, information on the connection between CSF and the cyst helps in determining prenatal intervention and postnatal management, including surgical treatment.
Differential diagnosis
The differential diagnosis of arachnoid cysts should include lesions that appear as intracranial hypoechoic lesions, such as porencephalic cysts, glioependymal cysts, aneurysms of the vein of Galen, schizencephaly, cystic neoplasms, and intracranial hemorrhage (ICH) [26].
Porencephalic cysts are fluid-filled structures of parenchymal origin. Thus, they are associated with parenchymal loss without a mass effect, which is a key component of differential diagnoses of arachnoid cysts (Fig. 2). Arachnoid cysts appear as fluid collections between the dura mater and the cerebral parenchyma and do not invade the underlying cortical ribbon and white matter [27]. Glioependymal cysts are very rare cysts found in various locations; when they exist extra-axially, it is difficult to differentiate them from arachnoid cysts. Both appear CSF-like on MRI and show no contrast enhancement. Therefore, histological examination is required for the differential diagnosis [28]. Aneurysms of the vein of Galen appear as an elongated anechoic lesion at the level of the cistern of the vein of Galen and can be distinguished from an arachnoid cyst by color and spectral doppler evidence of turbulent venous or arterial intraluminal blood flow (Fig. 3) [26].
Regarding schizencephaly, the most important differentiator is the presence of heterotrophic gray matter at the edge of the cleft. Such gray matter-lined clefts are not found in arachnoid cysts or other intracranial fluid spaces [29]. Cystic neoplasms, such as teratomas and astrocytomas, which contain a cystic portion, are distinguished from arachnoid cysts by the fact that their cystic components are solid and irregular [30]. Ultrasound findings of fetal ICH vary and are affected by location, time of occurrence, and severity. Because of this variability, ultrasound has less diagnostic value for fetal ICH, and fetal MRI is necessary to differentiate fetal ICH from other intracranial lesions [31].
Associated CNS and extra-CNS anomaly
According to a recent systematic review, an associated CNS anomaly was present in 74% of the patients with arachnoid cysts, and 14% had an extra-CNS anomaly [6]. The most commonly associated CNS anomalies are ventriculomegaly and callosal abnormalities [32]. Ventriculomegaly is present in 20-60% of these patients [8,19,33]. Although it may be caused by the mass effect of the cyst, which interrupts the flow of CSF, some authors have suggested a pathogenic association between arachnoid cysts and ventriculomegaly because CSF flow contributes to the development of arachnoid cysts [34]. Suprasellar or interhemispheric cysts in the supratentorial area are more likely to be associated with ventriculomegaly [19,33,35]. However, there is no association between cyst size and the presence of ventriculomegaly [19]. Callosal abnormalities are present in 10-40% of the patients [8,19,26] and are frequently associated with interhemispheric arachnoid cysts. Cysts in the interhemispheric space have been hypothesized to disrupt the development of the corpus callosum [36,37]. In addition, vermian abnormalities (including Dandy-Walker malformation and alobar holoprosencephaly) have also been reported [8].
No extra-CNS anomalies has been strongly associated with arachnoid cysts. However, this condition may accompany anomalies of various organs, including short femur length, cleft lip and palate, and heart anomalies [8]. Clinicians should also keep in mind that multiple anomalies may result from genetic abnormalities.
Genetic background
Most isolated arachnoid cysts are not associated with chromosomal abnormalities [6]. According to previous reports, chromosomal abnormalities were reported in 6-10% of the patients with arachnoid cysts [6,32], and all of these were accompanied by multiple structural abnormalities [6,8,26]. For instance, Pilu et al. [26] reported a case of Edward syndrome with a small arachnoid cyst, double-outlet right ventricle, and clenched hands. Souter et al. [38] reported unbalanced reciprocal translocation of chromosomes 14q and 20p in a case of midline arachnoid cyst, tetralogy of Fallot, and facial dysmorphism. Chromosomal abnormalities that have been reported in relation to arachnoid cysts include partial trisomy 9q and partial monosomy Xq [39], an unbalanced reciprocal translocation of chromosomes 14q and 20p [38], and trisomy 18 [26,40].
Familial inheritance of arachnoid cysts has been reported, although most arachnoid cysts are sporadic [41,42]. In a family with four family members affected by isolated intracranial arachnoid cysts in the same location, the array comparative genomic hybridization results revealed a maternally inherited 720-kb duplication of Xp22.2 that segregated with the disease phenotype in all affected individuals, but not in any of the unaffected family members [41]. In a family with six affected children from a consanguineous marriage in eastern Turkey, whole-genome linkage analysis demonstrated strong genetic linkage at chromosome 6q22.31-23.2.
One study from China reported an association between the elongator protein complex (ELP) 4 rs986527 polymorphism and the clinical features of arachnoid cyst [43]. ELP 4 is part of the multisubunit (ELP 1-ELP 6) extension complex, which is critical for the regulation of neuronal maturation (including neuronal system growth, development, and guidance) during neurogenesis. In a previous study of the three ELP 4 rs986527 genotypes in 85 patients with intracranial arachnoid cysts and 63 healthy control participants, the TC and C genotype frequencies were associated with a higher rate of neurological symptoms, including headache, epilepsy, and depression, than the TT genotype frequencies. C allele frequencies were associated with a higher rate of neurologic symptoms than T allele frequencies.
Antenatal changes and intrauterine treatment of arachnoid cysts
The size of arachnoid cysts can change during pregnancy. In previous studies, 75% showed no change in size, 20% increased in size, and 5% regressed [8,19]. The size change may differ depending on the location of the cyst. Arachnoid cysts on the skull base showed more progression than those in other locations [19], with a 50% increase in the volume of suprasellar cysts during pregnancy [33].
Some reports have investigated experimental treatment using fetoscopy when the cyst size increases rapidly [33,44]. Chalouhi et al. [44] reported that fetocisternoscopy with fenestration of the cystic wall cyst was successfully performed at 31 weeks in a fetus with a rapidly growing cyst. The baby was born at 36 weeks of gestation, underwent an additional cisternoscopy after birth, and maintained good health after surgery. The authors suggested that fetoscopic surgery might be an option in cases of rapidly growing intracranial arachnoid cysts. However, in utero treatment is not generally recommended.
Management during pregnancy
When an arachnoid cyst is first detected during pregnancy, detailed sonographic evaluation should be performed. The characteristics, size, and location of the cyst should be described to enable the differential diagnosis of other brain lesions, and other structural anomalies should be investigated [45,46]. Serial ultrasonography may be required to monitor cyst growth and progression of ventriculomegaly. According to the most recent study by Grossman et al. [16], prenatal follow-up imaging was performed 7 weeks after diagnosis. MRI helps detect associated anomalies and provides an accurate diagnosis [8,21,22]. MRI was preferably performed at 32 weeks to assess brain maturation and for a comprehensive scan of structures [17]. If other CNS or extra-CNS anomalies are identified, karyotyping and chromosomal microarray via amniocentesis should be considered [46].
Delivery is typically performed at term [17,26,32,47]. If the hydrocephalus becomes severe or acutely increases in size, delivery can be performed before term [8,47]. According to a recent systematic review, eight out of 69 women gave birth before term due to other intracranial abnormalities [32]. The delivery method can be chosen based on obstetric indications, and vaginal delivery is possible [4,17,19]. In previous studies, vaginal delivery was attempted and successfully performed [4,17,19]. In cases of cephalopelvic disproportion due to macrocephaly, cesarean section should be considered. A multidisciplinary treatment approach should be used, including an obstetrician, pediatric neurologist, and neurosurgeon who is familiar with management during both pregnancy and postnatal care in the management team.
Previous studies reported a pregnancy termination rate of 4-10%, most of which were due to genetic abnormalities and other anatomical abnormalities [4,17], although a study from China reported that 31/60 (52%) had a selective abortion, including four patients with an isolated cyst [8]. Because isolated cysts without associated abnormalities have shown favorable outcomes and the size of cysts or postnatal surgical intervention have not been significant predictors of poor outcomes [19,32], termination is not indicated by the diagnosis alone or the requirement for surgery after evaluating genetic and other anatomical abnormalities. An accurate diagnosis and a multidisciplinary team approach can avoid inappropriate pregnancy termination due to incorrect information.
Postnatal diagnosis and management
Arachnoid cysts should be confirmed after birth using MRI or ultrasonography because some cysts can either regress or worsen after birth. Cysts are not detected after birth in 10-40% of the patients [4,17]. In addition, careful examination should be performed to identify other congenital anomalies, macrocephaly, intracranial signs and symptoms, and visual and neuroendocrine symptoms.
Cyst size may also change during the postnatal period. In previous literature, 52-70% of the cases were stable in size, 20-24% progressed, and 10-24% regressed over time after birth [8,18]. Although the mechanisms for the spontaneous disappearance of arachnoid cysts have not been well described, several hypotheses have been proposed. A representative hypothesis is that the communication between the cyst and the subarachnoid space causes the cyst to disappear [48,49]. In addition, it is hypothesized that natural rupture of the cyst due to elevated intracystic tension by accelerating factors, such as crying or the Valsalva maneuver, may lead to cyst regression [50]. Another hypothesis is that the process of adhesion of the cyst wall due to head injury or infection may lead to the disappearance of arachnoid cysts [51].
Approximately 30-60% of the patients require surgical treatment after birth [6,19,32]. Half of the neonates who needed treatment underwent surgery soon after birth, while the rest underwent surgery several months later [19,32]. According to a recent systematic review, surgery was performed in 44% of the patients at 0-1 month, 40% at 1-6 months, and 15% after 6 months [32]. The reasons for surgery were ventriculomegaly or hydrocephalus (47%), cyst expansion (15%), and mass effect or intracranial pressure (ICP) elevation. In 87% of the patients with cyst progression in utero, surgery was required soon after birth. In addition, postnatal surgery may be associated with the cyst location. Most cavum veli interpositi cysts do not require surgery [6], and the operating frequency differs according to the location of suprasellar cysts [33]. In the decision to perform surgery, the patient’s neurological symptoms are more important than the size of the cyst. Surgery is indicated in children with neurological deficits related to cysts and increased ICP. Surgical treatment includes placement of a cystoperitoneal or ventriculoperitoneal shunt and cyst fenestration via endoscopy or open surgery. According to recent literature, of the patients who underwent surgery, 30% required a second surgery, and 5% required a third neurosurgical procedure [32].
The short-and long-term prognosis
Neonatal death occurred in 2.6% of the patients, all of whom had comorbid malformations or other genetic problems [5,32,47]. Representative postnatal complications include seizures and abnormal neurodevelopmental outcomes. Seizures were reported in approximately 5% of the patients; most of the patients who experienced seizures showed abnormal neurodevelopmental outcomes [32].
Generally, isolated arachnoid cysts are associated with favorable neurodevelopmental outcomes, although evidence for management is still lacking. In one study that evaluated 45 patients with a median follow-up of 4 years, 91% of the patients exhibited normal behavior, neurological development, and intelligence, and most of them were isolated cases [18]. In another study that investigated 20 patients over a median 2.5 years of follow-up, 80% of the children showed normal neurodevelopment, while 93% of those with an isolated cyst demonstrated normal neurodevelopment [8]. In another study that evaluated 22 patients for a median of 3 years follow-up, five patients (23%) had developmental delays [17]. Unlike in other studies, all patients with abnormal outcomes in this study were cases of isolated cysts. If these and other studies are combined, normal neurodevelopmental outcomes have been shown in 70-80% of all patients with arachnoid cysts and 90% of the patients with isolated cysts [6,8,17,32]. Neurodevelopmental outcomes are dependent on genetic factors and the presence of CNS or extra-CNS abnormalities rather than gestational age at diagnosis, cyst size, location, or need for surgery [19,32]. Additionally, visual impairment and growth hormone deficits associated with large suprasellar cysts have also been reported [4,33].








")











