



Introduction
Ultrasonography (USG) is an essential tool for the diagnosis, treatment, and monitoring of infertility in women. Transvaginal USG (TV USG) was first introduced in 1969 by Alfred Kratochwil [1] and has become one of the most valuable diagnostic modalities in the field of reproductive medicine worldwide. Compared with transabdominal USG, TV USG uses a high-frequency transducer focusing on the areas of interest, including the uterus, cervix, tubes, ovaries, cul-de-sac, and other organs within the pelvis. Therefore, TV USG is the standard method for diagnosing infertility, ectopic pregnancy, and abnormalities in the first trimester of pregnancy [2].
While greyscale USG provides information on the anatomy of the pelvis, color Doppler energy imaging provides information on its vascularity and functional aspects [3]. The Doppler modality allows for measurement of the direction and velocity of blood flow, which could be a marker for tissue hypoxia [4]. Doppler shift is the change in the wavelength or frequency produced by a moving source of waves relative to an observer [5]. This effect was first described by Christian Doppler, an Austrian mathematician and physicist, in 1842. A receding object produces lower-frequency echoes than an approaching object which produces higher-frequency echoes [6]. In 1955, Shigeo Satomura, a Japanese physicist, introduced ultrasonic Doppler techniques for medical diagnosis purposes and published the first measurement of the Doppler shift of ultrasound signals from various cardiac movements [7]. In 1985, Taylor et al. [8] were the first to publish a study showing that Doppler USG could be applied to examine ovarian and uterine blood flow. Since then, research on the use of Doppler USG in the field of gynecology has expanded and developed extensively.
Ultrasound waves are produced by the transducers and are perceived after collision with red blood cells within vessels when the color Doppler modality is used. A certain, or ŌĆ£gatedŌĆØ area of interest can be examined, which produces a velocity waveform from which the velocity or resistance of blood flow can be measured.
Peak systolic velocity (PSV): the tall peak of the waveform that represents the greatest velocity of the red blood cells in a vessel during systole [9]. The parameters that represent the resistance include [10]: systole to diastole (S/D) ratio: PSV/end-diastolic flow (EDF), pulsatility index (PI): (PSV-EDF)/mean velocity, resistance index (RI): (PSV-EDF)/PSV.
Color Doppler is less sensitive when examining small vessels or areas with slow blood flow. To overcome this, power Doppler can be used, which provides sufficient information about the quality and amount of blood flow per volume. Therefore, it is possible to predict the baseline vascular distribution of a target organ. Furthermore, 3-dimensional (3D) power Doppler allows for a more global assessment of total vascularity and is more precise when analyzing blood flow and quantifying the vascular distribution of the ovarian stroma [11]. Parameters of volume measurable by 3D power Doppler include vascularization index (VI), which represents the ratio of color information to all color and gray information in a given volume of interest; flow index (FI), which refers to the mean value of all color information in the vessels of the volume analyzed; and vascularization-flow index (VFI), which is measured by multiplying VI and FI; therefore, it can represent the general perfusion status in a given volume [12].
Numerous studies have been conducted on the application of color or power Doppler and 3D Doppler in the assessment of ovarian, endometrial, and uterine blood flow. Additionally, these modalities are sometimes used in clinical settings for the diagnosis and treatment of infertility. However, they are not utilized often and their use is mostly restricted to research. Here, the clinical use of Doppler USG is introduced, and some studies providing evidence of its efficacy are mentioned.
Ovarian blood flow
Ovarian vascular anatomy
Ovarian function is a very important factor in fertility, and it is known that the lower the ovarian function, the lower the egg quality [13]. The main blood supply to the ovary comes from the ovarian arteries, which originate directly from the abdominal aorta [14]. The ovarian artery enters the pelvis through the infundibulopelvic ligament near the pelvic brim and then passes inferiorly and medially between the two layers of the broad ligament, reaching the ovary via the mesovarium and passing through the ovarian hilum to give rise to multiple spiral branches. The ovarian artery is very tortuous, especially when it is close to the ovary [15]. The blood supply to the ovary also comes from the ovarian branch of the uterine artery, which joins with the ovarian artery, close to the ovary [16].
Follicular maturation and ovulation
Neovascularization within the ovarian stroma during the menstrual cycle is essential for the maturation of ovarian follicles and their normal function [17]. Using color Doppler USG, small vessels in the ovarian stroma and follicular rim can be detected, which allows for identification of the follicular maturation steps before ovulation [18]. Therefore, color Doppler for the identification of follicular maturation can be used to monitor patients undergoing infertility treatments such as timed coitus or intrauterine insemination (IUI).
Vascularity in the follicular rim first becomes visible or detectable when the follicle reaches 10 mm in diameter [19]. A mature follicle is approximately 16-18 mm in diameter, anechoic internally, and very thin-walled [20]. When color Doppler is applied, the vascularity surrounding the follicle is visible, and approximately 75% of its circumference is covered. Care must be taken not to mistake a stromal vessel very close to the follicle, and only if the color information overlaps with the follicular wall can it be considered a perifollicular vessel. A previous study showing the relationship between the percentages of follicular circumference and pregnancy rate reported that the group with a circumference of more than 75% showed significantly increased pregnancy rates [21]. Another study showed that perifollicular circumference of greater than 50% was related to increased oocyte retrieval rate, fertilization rate, and the number of grade 1 embryos [22].
When the follicle is close to ovulation, the vascularity increases on the inner wall of the follicle and usually shows a PSV value greater than 10 cm/s on pulse Doppler. A growing follicle needs more vascularization; therefore, the PSV rises, and the RI is steadily low, suggesting that the follicle is close to ovulation. This increase in PSV is attributable to the luteinizing hormone surge [23]. A lower PSV means that there is a lower blood flow supplying the follicle; therefore, it could represent the lack of follicular maturity. Likewise, an increased RI means that the resistance of blood flow is increased, and there is a lower blood flow during diastole to the follicles, which could also represent the lack of follicular maturity. A study by Nargund et al. [24] showed that fertilization of an oocyte from a follicle with a PSV of less than 10 cm/s led to a much lower chance of producing a high-quality embryo. Another study showed that an oocyte from a follicle with well-developed perifollicular vascularity and RI of Ōēż0.5┬▒0.05, which had a higher oxygen content, had a lower frequency of abnormalities in chromosomal organization on the meiosis-II spindle, and the embryos showed an increased ability to develop to the six-to eight-cell stage [25].
After ovulation, the dominant follicle collapses, and the vessels of the theca layer enter the follicular cavity [26]. At this point, blood flow increases, and good stromal vascularization can be seen on color Doppler USG. During the follicular phase, the ovarian artery has a low velocity with low diastolic flow, whereas during the luteal phase, there is increased blood velocity and reduced resistance. The RI starts to decrease 2 days before ovulation, remains low for 4 days after ovulation, and then slightly rises to a level of 0.5 in the mid-luteal phase, which is still lower than that in the follicular phase [27]. If pregnancy is achieved, the RI remains low at approximately 0.45 and continues to remain so during the first trimester until the luteal-placental shift occurs. Han et al. [28] showed that increased PI and RI in the blood flow surrounding the corpus luteum during the first trimester was associated with pregnancy termination. The meaning of Doppler that can be used clinically is summarized in Table 1.
Intrauterine insemination
During IUI treatment, monitoring follicle maturation on USG, deciding the time to trigger ovulation, and timing of insemination are important prognostic factors that affect the possibility of pregnancy. Previous studies have focused on whether the PSV level of individual follicles on the day of ovulation trigger affects assisted reproductive technology (ART) or pregnancy outcomes.
A study by Engels et al. [29] showed that the VI of the follicle did not differ significantly between ovulatory and anovulatory cycles and between cycles that did and did not achieve pregnancy. However, they found that periovulatory subfollicular VI and VFI were lower in pregnant women [29]. Another study by Panchal and Nagori [30] showed that pregnancy rates were higher when the perifollicular RI was <0.50, and the PSV was >11 cm/s on the day of IUI trigger. Furthermore, they found that perifollicular VI values between 6 and 20 and a perifollicular FI >27 led to higher pregnancy rates [30]. However, the findings remain controversial, and there are no definite references as to which vascularity parameters on the day of trigger increase the chances of pregnancy during IUI.
Controlled ovarian stimulation and in vitro fertilization
Ovarian blood flow has also been associated with gonadotropin dose requirement during in vitro fertilization (IVF) cycles. Higher blood flow to the ovary could lead to a higher concentration of gonadotropins being delivered to the developing follicles during controlled ovarian stimulation (COS) for IVF. Hence, it has been suggested that measuring ovarian blood flow using color or 3D power Doppler can predict the response to COS for IVF. The first study focusing on the relationship between ovarian blood flow and gonadotropin response was by Zaidi et al. [31], who showed that women with a poor ovarian response during IVF cycles had significantly lower ovarian PSV levels than normal responders. The adjusted odds of a poor ovarian response increased by approximately 22% per 1 cm/sec decrease in ovarian PSV. However, PI did not differ significantly between the two groups [30]. Likewise, Engmann et al. [32] showed that ovarian stromal PSV was the most important predictor of ovarian response during IVF treatment, and a PSV level of <10 cm/s was associated with a lower clinical pregnancy rate. In contrast, Ng et al. [33] showed that ovarian stromal blood flow indices measured by power Doppler USG had no predictive value for ovarian response.
Few studies have used 3D power Doppler to determine whether the ovarian response can be predicted in IVF cycles since 3D power Doppler could be used to measure and quantify the total blood flow to the ovaries. Kupesic and Kurjak [34] found that the total antral follicle count (AFC) and ovarian stroma FI showed the best predictive value for favorable IVF outcomes. Furthermore, the total ovarian volume and total ovarian stromal area measured using 3D USG also had high predictive values. Since 3D USG and Doppler are not invasive diagnostic tools, they claimed that they could be used without increasing the patientŌĆÖs discomfort and for a short time [34].
However, Merc├® et al. [35] reported that ovarian volume and AFC were the only predictors of the number of oocytes retrieved, but not the vascularity indices. Furthermore, none of the parameters were significantly different between the pregnant and non-pregnant groups [35]. A subsequent study by Jayaprakasan et al. [36] also reported that ovarian VI, FI, and VFI were similar in both normal and poor responders. Consequently, they concluded that ovarian blood flow measured using 3D Doppler USG is not predictive of response during IVF treatment [36]. There is insufficient evidence supporting the use of 3D Doppler USG in predicting IVF outcomes in the clinical setting, and further studies are still required.
Polycystic ovarian syndrome
Polycystic ovarian syndrome (PCOS) is a common but treatable cause of infertility in women. It represents approximately 80% of the cases of anovulatory infertility [37]. On ultrasound, a polycystic ovary is defined as an AFC per ovary of >20 and/or an ovarian volume Ōēź10 mL [38]. Ovarian blood flow assessment using Doppler USG is not required to diagnose PCOS; however, few studies have attempted to measure ovarian vascularity using color or power Doppler USG.
According to Ozkan et al. [39], ovarian artery PI, RI, and systole to diastole ratios were significantly lower in women with PCOS. However, a study by Tugrul et al. [40] showed similar mean PI values in the ovaries of women with PCOS and in control groups and therefore stated that it is not beneficial to use color Doppler USG in the clinical diagnosis of PCOS.
The results regarding ovarian blood flow and volume measured using 3D power Doppler in PCOS patients are also controversial. Pan et al. [41] showed that women with PCOS had a higher mean ovarian volume, VI, FI, and VFI of the entire ovarian stroma, using 3D power Doppler. In contrast, Ng et al. [42] showed that infertile women with PCOS had similar total ovarian VI/FI/VFI as fertile controls on 3D power Doppler.
Uterine blood flow
Uterine vascular anatomy
The blood supply to the uterus comes mainly from the uterine artery, which arises from the anterior division of the internal iliac artery [14]. It runs medially in the pelvis inside the base of the broad ligament, and within the broad ligament, the uterine arteries are divided into descending and ascending portions. The ascending branches run alongside the uterus and pass anteriorly to the ureter. Within the uterus, the uterine arteries branch further, giving rise to radial arteries, which arise from the arcuate arteries and are directed toward the endometrium, which then become spiral arteries [43]. Some of the blood supply to the uterus comes from the ovarian arteries, which anastomose with the superior branches of the uterine arteries within the broad ligament [15].
Uterine artery doppler
Many studies have measured the uterine arteries to assess blood flow to the uterus because it is easily accessible compared with its smaller branches. Uterine blood flow plays an important role in controlling endometrial growth and is thought to be closely related to vascularity of the endometrium [44]. However, when measuring the vascular indices of the uterine artery, caution must be exercised when interpreting the results, as these might not be representative of the actual blood supply to the endometrium.
The uterine artery Doppler waveform in the non-pregnant state shows a rapid rise in systolic flow and a sudden fall, followed by a notch during early systole [45]. However, this high impedance progressively disappears during pregnancy [46]. During the normal menstrual cycle, the flow changes periodically. There are increases in PI values and blood flow velocity during the early follicular phase, which are maximal at the mid-luteal phase. A few studies have shown a decrease in PI 1 week before and after ovulation [47,48]. The RI is about 0.88┬▒0.04 in the proliferative phase and starts to decrease the day before ovulation. It decreases to 0.84┬▒0.04 on the 18th day of the menstrual cycle, and remains at that level for the rest of the cycle. These changes do not occur during anovulatory cycles [49]. Such a decline in uterine artery resistance during the mid-luteal phase has been suggested to reflect optimal vascularity for embryo implantation [50].
Several studies have been carried out to assess the association between uterine artery vascular parameters on color or power Doppler USG and the outcome of IVF and embryo transfer (ET) cycles. Cacciatore et al. [51] showed that PI and RI indices were lower in the conception cycles, and the pregnancy rate after ET declined when PI was >3.3 and RI >0.95. Similarly, in another study, the uterine artery PI and RI were significantly increased and the subendometrial VI, FI, and VFI were significantly decreased in the unexplained infertility group, suggesting that peri-implantation uterine perfusion is impaired in women with unexplained infertility [52]. Furthermore, Coulam et al. [53] reported that a PI value >3.3 on the day of ovulation trigger had a negative predictive value of 88% for pregnancy. However, a later study by Hoozemans et al. [54] found that serial Doppler ultrasound examination of the uterine artery did not differ between women who underwent IVF-ET cycles, resulting in ongoing pregnancy, miscarriage, or no pregnancy.
Radial artery Doppler
The measurement of blood flow in the uterine radial artery has received increased attention because the radial artery crosses the myometrium and is therefore considered to reflect the endometrial blood flow more accurately. A study by Tamura et al. [55] showed that radial artery RI remained at the late luteal phase level until the 5th week of pregnancy, then significantly decreased until the 7th week and remained low until the 10th week. The RI of the uterine artery remained at the late luteal phase level until the 10th week and decreased gradually until the 16th week [55]. Such a decrease in the RI of the radial arteries occurs due to the vascular remodeling present at the site of placentation, causing a reduction in local arterial resistance [56].
Koo et al. [57] reported that the RI levels of the uterine radial artery were higher in pregnant women with recurrent pregnancy loss than in controls, and these women showed a positive correlation with RI levels and peripheral blood natural killer cell fractions. A subsequent study by the same team showed that the uterine radial artery RI during the early follicular phase was significantly lower in the pregnant group than in the non-pregnant group. In addition, the difference in the changes in the uterine radial artery RI from the pre-ovulatory to mid-luteal phase between the two groups was significant. In the pregnant group, the RI decreased, while it did not in the non-pregnant group. Therefore, they concluded that increased endometrial flow in terms of radial artery RI during the mid-luteal phase may correlate with successful IVF-ET outcomes [58].
Endometrial blood flow
Endometrial vascularity and morphology
The uterine radial arteries run through the myometrium just outside the endometrium, where they form terminal branches that are straight and coiled. Straight branches are the basal arteries that supply the basal layer of the endometrium. The coiled branches are spiral arteries that cross the endometrium and supply the functional layer [14].
The endometrium thickens during the menstrual cycle and undergoes morphological changes in response to increasing estrogen levels produced by the development of ovarian follicles. This is also associated with the increased vascularity of the spiral arteries developing along the functional layer [59]. The vascularity of the endometrial changes can be detected on color Doppler USG, although some investigators are unable to replicate the same findings.
Spiral artery Doppler
Blood flow in the uterine arteries may not necessarily pass through the endometrium. Therefore, it seems more reasonable to measure the vascularity of the endometrium and the surrounding vessels to assess its association with endometrial receptivity and pregnancy outcomes. This can be achieved by measuring the vascular indices of the spiral arteries of the sub-endometrium. Studies assessing the blood flow in the spiral arteries showed similar patterns of blood flow in the uterine arteries during the menstrual cycle. The RI of spiral arteries remains high in the follicular phase and decreases rapidly to a level of 0.48 3 days before ovulation [19]. On 3D Doppler, the VI, FI, and VFI increase from the midfollicular phase, peaking 3 days before ovulation, and then decrease, reaching a nadir 5 days post-ovulation, before gradually increasing again during the mid-luteal phase [60].
Endometrial-subendometrial blood flow and assisted reproductive technologyoutcomes
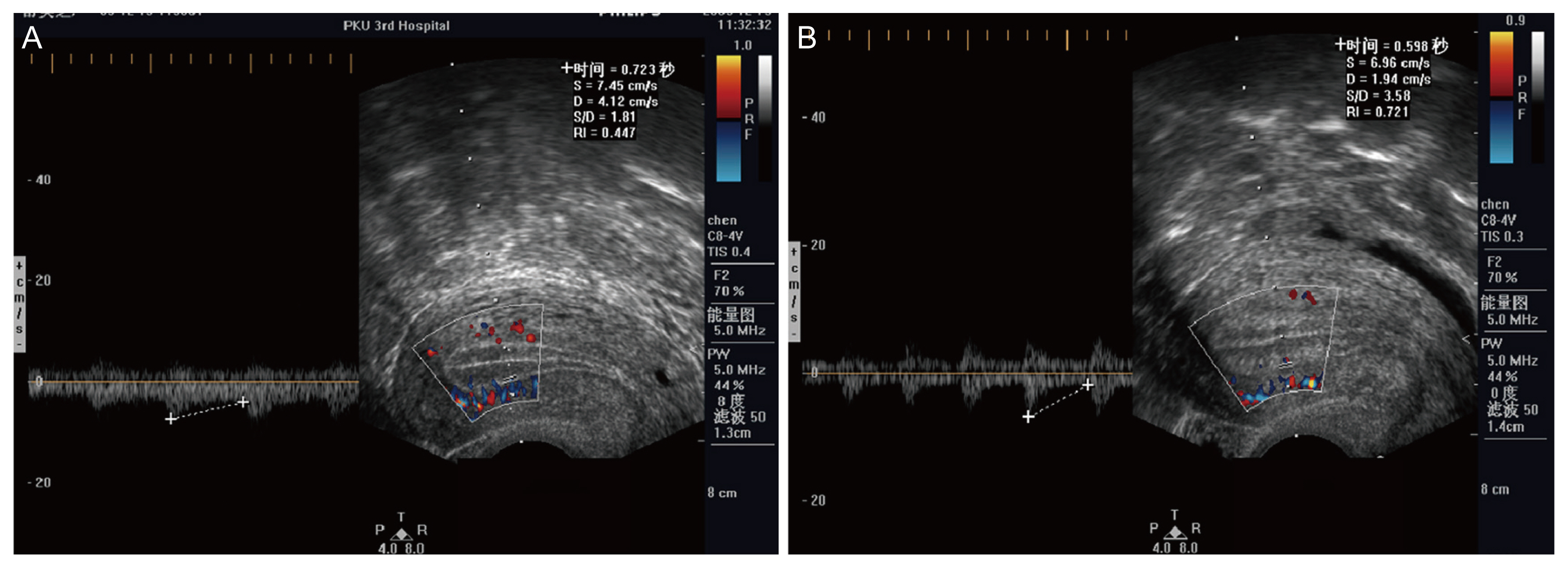
Color Doppler assessment of endometrial blood flow has been positively associated with pregnancy outcomes. Wang et al. [61] investigated whether the presence of endometrial blood flow, subendometrial blood flow, or both affected pregnancy in women undergoing IVF-ET cycles (Fig. 1). They found that the group with both endometrial and subendometrial blood flows had higher pregnancy and implantation rates. The S/D ratio, PI, and RI of the spiral arteries measured on the day of the trigger were significantly lower in patients with a successful pregnancy [61] (Fig. 2). Kupesic et al. [62] found the same when measuring the color Doppler of the endometrium on the day of ET. Similarly, Chien et al. [63] found that the presence of both endometrial and subendometrial blood flow was an indicator of good endometrial receptivity. They also showed that when pregnancy is achieved in the absence of endometrial and subendometrial flow on the day of ET, more than half of these pregnancies would finish as spontaneous miscarriages [63]. In contrast, a study by Nandi et al. [64], which focused on frozen ET cycles, found no significant differences in the endometrial and subendometrial vascular parameters measured by 3D power Doppler between those who did and did not manage to become pregnant.
In the case of IUI, Kim et al. [65] showed that the endometrial VI, FI, and VFI scores were significantly higher on the day of IUI in women who achieved pregnancy. However, subendometrial vascular parameters were similar. Omran et al. [66] showed that using clomiphene citrate in women with unexplained infertility led to decreased endometrial VI, FI, VFI, and subendometrial VI, FI, and VFI. Therefore, peri-implantation endometrial perfusion is lower in clomiphene citrate-stimulated cycles [66].
Furthermore, Ng et al. [67] found that patients with hydrosalpinx had significantly lower endometrial and subendometrial VI and VFI, suggesting that decreases in endometrial and subendometrial blood flow may be the reason for impaired implantation in patients with hydrosalpinx.
Combining the evidence showing a positive correlation between Doppler USG findings and ART outcomes, AppelbaumŌĆÖs uterine scoring system for reproduction (USSR) was devised. The USSR is a scoring system for the following parameters: endometrial thickness, endometrial layering, endometrial motion, uterine artery Doppler flow evaluated by PI, endometrial blood flow within zone 3, and myometrial blood flow [68]. Subsequent studies found that USSR is highly indicative of good pregnancy outcomes in patients undergoing intracytoplasmic sperm injection and ET [69].
Nevertheless, regarding endometrial vascular parameters measured on Doppler examinations and the outcomes of ART, the results are still inconsistent, and further large-scale studies are required. Therefore, care must be taken when interpreting Doppler examination results in routine clinical settings to assist in the management of infertility patients.
Conclusion
Doppler ultrasound investigations of female infertility include the examination of ovarian, uterine, and endometrial blood flow. Both color or power Doppler and 3D power Doppler have important roles in research settings, but their roles in clinical settings remain limited. A large amount of evidence from such examinations is mounting, and its use to assist in the management of infertility patients seems promising. Numerous studies have shown a correlation between the blood flow of the ovaries, uterus, and endometrium and pregnancy or ART outcomes in female infertility. However, the conclusions of this study are inconsistent. This may be because measuring the Doppler parameters of the perifollicular vessels, uterine artery, radial artery, spiral artery, and others may not reflect the blood flow to the endometrial or ovarian follicles. However, the technology of Doppler USG is advancing rapidly, which may lead to improved and consistent examination of blood flow to the endometrial or ovarian follicles. This will allow for the use of color or power Doppler and 3D Doppler in routine clinical practices in the future to accurately predict the outcome of ART and to improve the management of infertility patients, leading to better pregnancy outcomes.







")











