Preoperative modified frailty index to predict surgical complications in endometrial cancer patients
Article information

Abstract
Objective
To assess the predictive value of the preoperative modified frailty index (mFI) for postoperative complications in endometrial carcinoma, evaluate risk factors associated with complications, and compare the predictive properties of the mFI with the American Society of Anesthesiologists (ASA) physical status classification.
Methods
A total of 364 patients with endometrial cancer who underwent primary surgery between January 2009 and December 2016 were examined. The prognostic value of mFI in predicting severe postoperative complications, assessed according to the Clavien-Dindo classification, was analyzed and compared with ASA status. The risk factors for adverse outcomes were determined using multivariate analysis.
Results
The 30-day postoperative surgical- or medical-related complication rate was 26.6%. The rates of postoperative complications were 1.3%, 8.8%, 12.2%, and 60.0% for mFI scores of 0, 1, 2, and ≥3, respectively (P<0.001). The odds ratios for predicting postoperative complications in patients with mFI scores of 1, 2, and ≥3 were 7.38, 10.59, and 114.75, respectively. In the multivariate analysis, the significant predictive factors for postoperative complications were mFI ≥1, body mass index (BMI) ≥30 kg/m2, and non-endometrioid cell type. At cut-off points of mFI ≥1 and ASA ≥2, both tools had similar sensitivities but mFI was more specific (sensitivities 92.9% vs. 100%; specificity 45.5% vs. 19.4%).
Conclusion
mFI provides a satisfactory predictive value for postoperative complications. Patients with an mFI score ≥1, a BMI ≥30 kg/m2, and a non-endometrioid subtype, are at risk of postoperative complications and should receive comprehensive preoperative and postoperative management.
Introduction
Endometrial cancer is the most common gynecological cancer in developed countries [1,2] and the second most common cancer in developing countries [1]. In Thailand, endometrial cancer is the third most common genital tract cancer after cervical and ovarian cancers, and its incidence is on an increasing trend [3,4].
The current standard of treatment for endometrial cancer is surgery. The postoperative complication rate among patients with endometrial cancer undergoing primary surgery is 16.2–37.9% [5–7]. Patients who develop complications have decreased long-term survival and require alternative treatment modalities [8]. Prediction and early detection of surgical complications may improve adverse outcomes and survival rates.
Recently, many scoring systems have been developed to more precisely quantify the likelihood of postoperative complications. Examples of scoring systems used for these purposes include the American Society of Anesthesiologists (ASA) physical status classification system, acute physiology and chronic health evaluation, physiologic and severity score for the enumeration of mortality and morbidity [9], and the prognostic nutritional index [10]. The accuracy of scoring systems in predicting complications varies considerably across patient populations. Thus, the indications for surgery and surgical procedures for their general use are limited. Although many possible risk factors for postoperative morbidity and mortality have been extensively analyzed, uncertainty remains regarding which patients will have adverse outcomes in the postoperative period [10–12], especially among the older adults, who generally carry a higher risk of surgical morbidity and mortality [13].
The frailty index is a model developed based on a comprehensive geriatric assessment of the overall decline in function, which is explained by the additive effects of comorbidities [14]. The first frailty index reported by Rockwood et al. [15] comprised 70 variables that were used to calculate the score. A higher score on this index indicates greater frailty. The modified frailty index (mFI) [16] was developed from the Canadian study of health and aging frailty index, using a cumulative deficit model simplified from the original frailty index. mFI is less time-consuming for both physicians and patients because it incorporates 11 items and provides a more practical assessment because of the feasibility of data collection. A previous study demonstrated that mFI had more predictive power than ASA in terms of both morbidity and mortality [17,18].
mFI has recently emerged as an important tool in general surgery and surgical specialties for the evaluation of perioperative risk in older patients [16,19–22]. Uppal et al. [21] found that mFI predicted the need for critical care support and 30-day mortality after surgery for gynecological cancer. This study aimed to assess the predictive properties of the preoperative mFI concerning postoperative morbidity and mortality, identify the risk factors associated with postoperative complications, and compare the predictive properties of mFI with those of the ASA score.
Materials and methods
We retrospectively examined patients with endometrial cancer who underwent surgical staging at the Songklanagarind Hospital between January 2009 and December 2016. Patients with endometrial cancer, aged 50–90 years and treated with surgical staging as the primary treatment were included; those who had previously undergone chemotherapy or pelvic radiotherapy were excluded. All patients included in the study provided written consent for data collection and the use of personal records for health research. This study was approved by the Human research ethics committee of the faculty of medicine at prince of Songkla University.
mFI scores were calculated for each patient (Table 1) [16]. A score of 0 was the lowest possible score (0 positive items out of the 11 total items), signifying the absence of frailty, whereas a score of 11 was the highest possible score (11 positive items out of the 11 total items), equivalent to maximum frailty.

The occurrence of postoperative complications was subsequently recorded for each patient, along with information detailing the number of complications that occurred within 30 days postoperatively and the severity of complications that occurred using the Clavien-Dindo classification, which is a grading system based on the magnitude of the interventions required to manage the complication and whether the complication causes permanent disability or death [23,24]. The patients were classified as having no or minor (Clavien-Dindo grade I–II) complications or severe (Clavien-Dindo grade III–V) complications that required some type of intervention.
The sample size was calculated using infinite population proportions, which was 350 patients. Statistical analysis was performed using the R software version 3.3.0 (R Foundation for Statistical Computing, Vienna, Austria). The occurrence of severe complications was analyzed in comparison with the mFI score using univariate analysis with the chi-squared test. Multivariate logistic regression was performed to identify the variables affecting 30-day postoperative complications. The rates of severe complications by ASA class and mFI score were determined using the receiver operating characteristic (ROC) curve to detect the sensitivity, specificity, and area under the curve (AUC) of each tool. The DeLong’s test was used to compare the differences in the areas under the two ROC curves. The statistical significance level was set at P<0.05.
Results
During the study period, 364 patients with endometrial cancer underwent surgical staging. The patient characteristics are summarized in Table 2. The mean age of the study participants was 60 years (range, 50–87), and the median body mass index (BMI) was 27.2 kg/m2 (range, 13.0 to 48.5 kg/m2). Ten patients (2.7%) had Clavien-Dindo grade III–V complications.
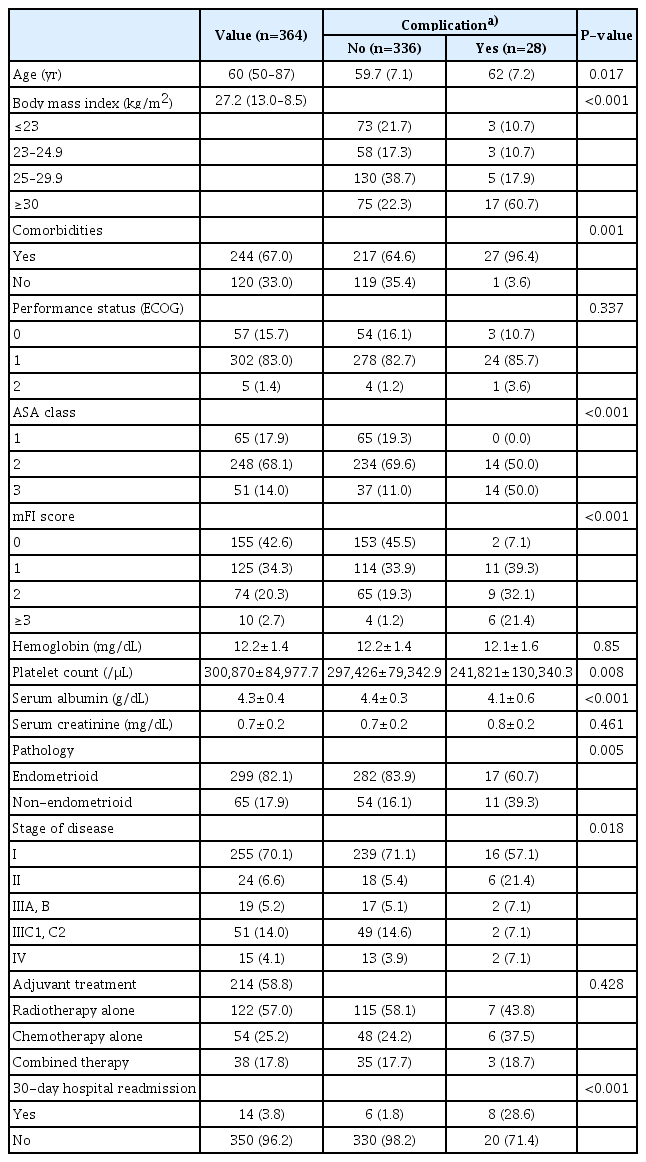
Patient characteristics
The frequencies of the mFI scores were as follows: 1) 155 patients (42.6%) with a score of 0; 2) 125 patients (34.3%) with a score of 1; 3) 74 patients (20.3%) with a score of 2; 4) eight patients (2.2%) with a score of 3; and 5) two patients (0.6%) with a score of 4. The rates of Clavien-Dindo grade III–V complications (Table 3) were 1.3%, 8.8%, 12.2%, and 60% for mFI scores of 0, 1, 2, and ≥3, respectively (odds ratios [OR] were 7.38, 10.59, and 114.75 [mFI score of 0 as reference], respectively).
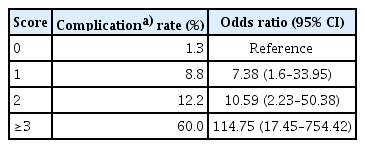
Modified frailty index score and Clavien grade ≥III complications
Ninety-seven patients (26.6%) had postoperative complications. The common complications were 1) wound infection in 52 cases (14.3%); 2) vaginal stump infection in 17 cases (4.7%); 3) urinary tract infection in eight cases (2.2%); and 4) partial gut obstruction, lung atelectasis, diarrhea, and hyperglycemia in three cases (0.8%). Clavien-Dindo grade III–V classification was determined in 28 cases (7.7%), and surgical wound infections were the most common complications (24 cases [85.7%]). One patient died of cardiac arrest during the operation (this patient had an ASA score of class III and an mFI score of IV).
A comparison between the mFI and ASA scores to predict Clavien-Dindo grade III–V complications showed that mFI had an AUC (AUC, 0.76) similar to that of ASA (AUC, 0.74) in predicting complications (P=0.75). At the cut-off points of mFI ≥1 and ASA ≥2, the sensitivities and specificities were 92.9% (95% confidence interval [CI], 75.0–98.8), 45.5% (95% CI, 40.1–51.0), 100% (95% CI, 85.0–100.0), and 19.4% (95% CI, 15.3–24.1), respectively.
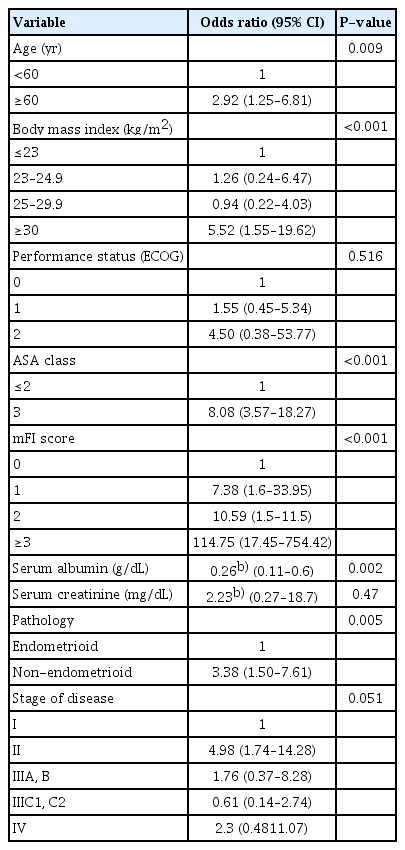
Univariate analysis revealed that age ≥60 years, a BMI ≥30 kg/m2, an ASA score >2, an increased albumin level, a non-endometrioid cell type, and an mFI score ≥1 were significant risk factors for severe complications (Table 4). However, only mFI score ≥1, BMI ≥30 kg/m2, and non-endometrioid cell type remained significant predictors of Clavien-Dindo grade III–V complications in multivariate analysis (Table 5).

Discussion
Recent studies in patients undergoing general surgery have suggested that perioperative morbidity and mortality can be predicted using preoperative assessment tools. In our study, we examined mFI as a predictor of postoperative complications in patients undergoing surgery for endometrial cancer. We demonstrated that the mFI score was associated with an increased risk of developing postoperative complications.
Although there are several methods to measure frailty, there is no clear agreement regarding the most appropriate method. The mFI-11, one of the tools available for measuring frailty, uses the scores of accumulating deficits to identify postoperative morbidity. mFI-11 was designed to analyze data from 2006 to 2016 from the Songklanagarind Hospital Program database. A new mFI (mFI-5) that is as effective in predicting mortality and postoperative complications as mFI-11 has been adopted since 2017. However, the years of collecting data limited our study.
Frailty is defined primarily in people aged over 60 years as a decrease in physiologic reserves and multi-organ function and is different from the normal aging process or that it addresses this exact age. Endometrial cancer predominantly affects postmenopausal women and is uncommon in women aged <50 years. In our study, patients older than 50 years of age, during which natural menopause occurred, were included.
A previous report by Uppal et al. [21] showed that an mFI score of 3 or ≥4 was associated with a significant increase in the rate of combined Clavien-Dindo grade IV and V complications (P<0.001). Velanovich et al. [19] reviewed 971,434 surgeries in a wide variety of surgical subspecialties, including cardiac, general, gynecologic, and neurosurgical, from the national surgical quality improvement program database. They found a direct variation between the mFI score and morbidity and mortality rates because each specialty and level of operation complexity (trend of odds P<0.0001 for all comparisons) resulted in a gradual increase in both morbidities, with an odds ratio (OR) of 1.24–3.36, and mortality, with an OR of 1.33–46.33. Our study adds further support to the understanding that increased frailty, as measured using mFI, is associated with significantly greater odds of developing a higher Clavien-Dindo grade complication.
Our series indicated that mFI scores of 1, 2, or 3 were associated with postoperative complications in patients with endometrial cancer who underwent primary surgery (ORs 5.16, 8.75, and 105.83, respectively). Uppal et al. [21] found that postoperative complications in gynecologic cancer patients increased (ORs 1.91, 2.33, and 12.5 for mFI scores of 2, 3, and 4, respectively). The dissimilarity in the strength of the association may be explained by the differences in the severity of comorbidity, surgical complexity, and quality of medical care.
We found that an mFI score ≥1, BMI ≥30 kg/m2, and non-endometrioid cell type were significantly associated with postoperative complications in multivariate analysis. A higher mFI score resulted in increased postoperative complications because the sum of the scores represented multiple comorbid conditions. Surgery for patients with multiple comorbidities puts them at a high risk. Obesity is associated with postoperative complications from microvascular abnormalities because excessive adiposity contributes to obesity-related microangiopathy and a progressive increase in proinflammatory cytokine production resulting from the activation of natural killer cells by excess lipids and other inflammatory mediators, including angiotensinogen, tumor necrosis factoralpha, leptin, interleukin 6, and transforming growth factor-beta [25]. Surgery for the non-endometrioid cell type was significantly associated with severe postoperative complications compared with other cell types.
Our study evaluated the use of mFI in perioperative risk prediction in comparison with the ASA physical condition classification system, which is used to evaluate patients’ pre-anesthetic medical comorbidities. The ASA classification is subjective and based on multiple age-independent factors that are accepted by most practitioners. Our study limited the age range to 50–90 years to ensure that the majority of endometrial cancers were included. We demonstrated that mFI might have a better predictive property than ASA. At the best cutoff point of each model, both tools had similar sensitivities but mFI had better specificity (sensitivity, 92.9% vs. 100%; specificity, 45.5% vs. 19.4%), with an mFI ≥1 and ASA ≥2. We selected mFI ≥1 and ASA ≥2 as the best cutoff points for each tool based on their high sensitivity and acceptable specificity to achieve the value of the screening test. Multivariate analysis also supported that the mFI score, but not the ASA score, is a prognostic factor for severe postoperative complications. Our results were similar to those of previous studies by Farhat et al. [17] and Adams et al. [18], who found that mFI was a better predictor of morbidity and mortality rates than ASA using multivariate logistic regression analysis. The ASA score is based on a subjective assessment of the degree of comorbidity before surgery rather than the “operative risk” [26,27]. The ASA score has also been criticized for its lack of accuracy and inconsistencies among evaluators [28].
This is the first study to evaluate the predictive value of preoperative mFI in gynecologic cancer patients by reducing the heterogeneity in patient selection and using uniform treatment. However, this study has some limitations. First, this study was retrospective in nature, and longitudinal follow-up data after 30 days was unavailable. Second, the surgical complexity varied widely, depending on the comorbidity, staging, and histologic subtype of each patient and the surgeon’s technical skill; therefore, among patients with the same score, there may have been disease severity heterogeneity that was not accounted for in the model. In the future, we suggest a prospective study to determine whether the use of a predictive model alters postoperative outcomes and survival, and a new tool that is feasible and incorporates the details of the severity of comorbidities into the model should be developed.
In conclusion, mFI provides a predictive outcome for 30-day postoperative complications. Patients with an mFI score ≥1, a BMI ≥30 kg/m2, or a non-endometrioid cell type are at a higher risk of postoperative complications. Utilizing mFI can more effectively identify high-risk patients, yield a valuable tool for patient and family counseling, and offer intensive preoperative and postoperative management.
Acknowledgments
The authors would like to thank the Department of Obstetrics and Gynecology, Prince of Songkla University, for providing us with the opportunity to perform this study.
Notes
Conflict of interest
The authors declare that there are no conflicts of interest.
Ethical approval
This study was approved by the Human Ethics Committee of the Faculty of Medicine, Prince of Songkla University.
Patient consent
All authors confirm that all patients provided written informed consent for the inclusion of material pertaining to themselves and that the authors have fully anonymized them.
Funding information
None of the authors received any specific funding.