Role of interleukin-6 (IL-6) in predicting gestational diabetes mellitus
Article information

Abstract
Gestational diabetes mellitus (GDM) is the most common pregnancy-associated metabolic disorder that is steadily increasing worldwide. Early diagnosis of pregnant women susceptible to GDM is the first step for deploying effective preventive treatment to reduce maternal, fetal, and neonatal complications. The diagnostic process of GDM is still controversial and interleukin-6 (IL-6) is one of the most recent markers used for the diagnosis of GDM. In this study, we aimed to systematically review the role of IL-6 in the diagnosis of GDM. In this systematic review, Google Scholar, Scopus, PubMed, ISI Web of Science, ProQuest, and MEDLINE databases were searched using the following keywords: GDM, screening, and IL-6, with the time interval 2009–2020. The quality of articles was assessed using the Strengthening the Reporting of Observational Studies in Epidemiology checklist. Twenty-four articles with desired quality that met the inclusion criteria were selected and reviewed further. Sixteen studies showed a statistically significant association, while 8 studies did not report any relationship between IL-6 levels and GDM. Based on the results of these studies, assessing the serum IL-6 levels can be investigated a newly established diagnostic biomarker for GDM. Therefore, through early diagnosis of susceptible women, effective measures can be implemented to reduce its complications.
Introduction
Diabetes is a metabolic disorder with steadily increasing prevalence. By 2014, 422 million adults were reported to have diabetes and at least 629 million people will be affected by 2045 if appropriate measures are not taken to reduce it. It has also been reported that high blood sugar causes 4 million deaths each year. The effects of diabetes go beyond the individual level, as it also affects the family and society and have wide-ranging socio-economic consequences [1]. Gestational diabetes mellitus (GDM) is a type of Diabetes, which is defined as diabetes diagnosed during the second or third trimester of pregnancy without prior detection [2]. GDM is a heterogeneous disorder resulting from the interactions between environmental and genetic factors [3]. Obesity and advanced maternal age are associated with the increasing prevalence of GDM worldwide. GDM heightens the potential risk of type 2 diabetes onset in the mother and her offspring [4]. The prevalence of GDM worldwide is estimated to be 17%, varying across different regions, with an estimate of 10% in North America and 25% in Southeast Asia [5].
GDM is associated with adverse pregnancy outcomes, including preeclampsia, polyhydramnios, fetal macrosomia, stillbirth, and neonatal complications such as hypoglycemia, hyperbilirubinemia, hypocalcemia, polycythemia, and respiratory distress [5]. Consequences of GDM extend beyond infancy and pregnancy, increasing the risks of metabolic syndrome, impaired glucose tolerance, and obesity in the offspring of affected mothers; it is a robust marker for the diagnosis of type 2 diabetes and diabetes-associated vascular diseases for the mother [6]. Various studies have shown that the lifestyle changes during pregnancy, especially in the early stages of pregnancy, can help in reducing the risk of GDM and also improve the adverse consequences associated with it [7].
Pregnancy represents a complex metabolic and physiological state in women. Insulin resistance plays a crucial role in the pathophysiology of GDM; in normal pregnancy, it can occur due to the increased secretion of diabetogenic placental hormones [8]. Despite over five decades of research, a common consensus on an internationally accepted screening method for GDM is yet to be achieved. Disagreements include the optimal time for screening, appropriate screening test, and general or selective screening methods [9]. According to World Health Organization (WHO), GDM can now be diagnosed with gestational glucose tolerance test using 75 grams of glucose at 24–28 gestational weeks [10]. Oral glucose tolerance test (OGTT) is an unpleasant test requiring consumption of 75 grams of glucose and delaying gastric discharge, which can cause nausea and vomiting. It is also a time-consuming method that requires overnight fasting before collection of 3 blood samples [11]. Moreover, an increase in the maternal blood glucose and fetal growth pathway occurs before 24 weeks of gestation, which has not been diagnosed in GDM. Early diagnosis of pregnant women with GDM and timely treatment can reduce the short- and long-term complications associated with it [12]. Researchers are currently investigating various markers to diagnose GDM, including interleukin-6 (IL-6) [13]. IL-6 is a cytokine produced by immune, adipose, and endothelial cells, and can have significant effects on glucose metabolism. IL-6 also affects pancreatic islet beta cells and enhances insulin secretion [14]. Additionally, inflammatory markers such as IL-6 have also been implicated in the pathogenesis of type 2 diabetes [15].
Numerous studies have been conducted on the association of IL-6 with GDM. Some studies have shown a statistically significant association between elevated IL-6 levels and GDM [4,13,16], while others did not report such relationships [17,18]. To this end, considering the contradictory results regarding the association between IL-6 and GDM, and based on the literature, there is no systematic review discussing the association between IL-6 and GDM. Therefore, in this systematic review, we aimed to investigate the association between IL-6 and GDM.
Methods
1. Search strategy
This study was conducted based on the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses. In order to collect data in a systematic manner, reliable databases such as MEDLINE, ISI Web of Science, PubMed, Scopus, Google Scholar, and ProQuest were used (Table 1).

Search strategy
2. Inclusion and exclusion criteria
Inclusion criteria included all the observational articles published in English and Persian from January, 2009 to February, 2020, in which the healthy pregnant women were in the age group of 18–40 years and screened for gestational diabetes during 24–28 gestational weeks.
Lack of access to the full text of articles, protocol studies, case studies, brief reports, all non-Persian and non-English articles, as well as studies on high-risk pregnant women (over 40 years of age, with body mass index (BMI) over 30, family history of type 2 diabetes, history of polycystic ovary syndrome, thyroid problems, hypertension, diabetes, and tobacco use, and any other disorders affecting the maternal and neonatal health) were excluded.
3. Study selection
In the initial search, 2,578 articles were fetched. Two different researchers reviewed these articles and disagreements were resolved by a third one. Subsequently, 1,478 duplicated articles were removed. After reviewing the titles and abstracts, 900 more articles were excluded. After reviewing the full text of the articles in the next step, 100 articles were removed due to incompetence. Finally, 24 articles were considered sufficiently qualified and eligible for further reviewing (Fig. 1).
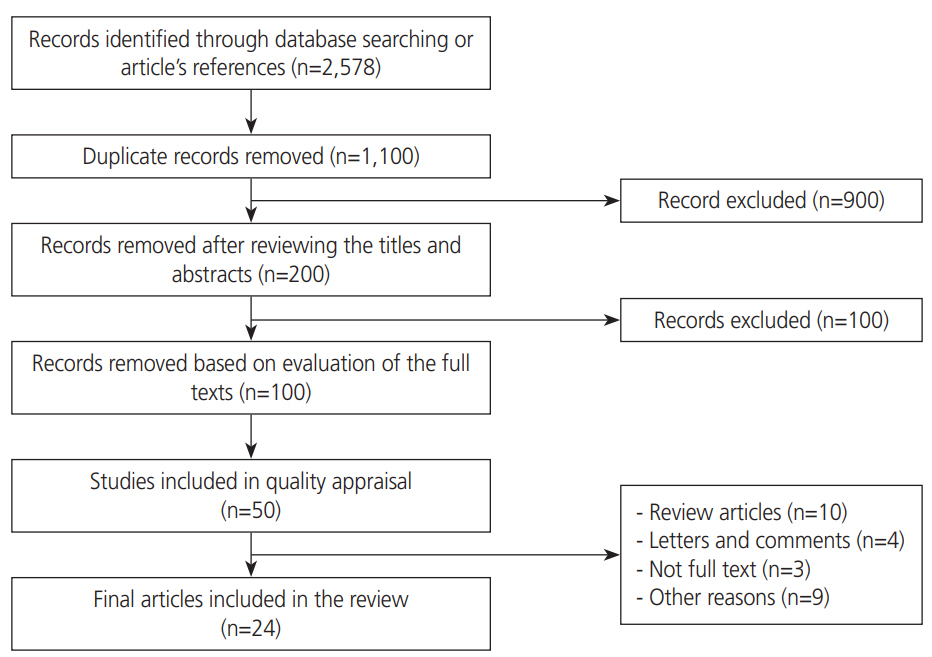
Flow diagram for searching the articles.
4. Quality assessment
Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statements were used to assess the quality of the studies. The STROBE statement as a valid tool consists of a checklist of 22 items to assess the quality of different parts of the observational studies [19,20].
5. Data extraction
Initially, the selection and evaluation of studies were performed independently by the 2 researchers, and the disagreements were resolved by a third one. Information on the first author’s name, year of publication, geographic region, study design, participants, BMI, sample, test time, test analysis method, diagnostic criteria of GDM, and levels of IL-6 were extracted and considered for the analysis.
Results
According to the process of search for articles, flowchart of which is presented in Fig. 1, 24 relevant high quality articles were selected and considered in this study after thoroughly reviewing the selected articles. Quality of the selected articles was assessed on the basis of the STROBE checklist (Fig. 2). These studies included articles published from 2009 to 2020, which were mainly case-control (n=17), cross-sectional (n=2), observational (n=2), cohort (n=2), and longitudinal (n=1) studies. A total of 2,806 pregnant women participated in these studies and blood samples were collected for measuring IL-6 levels in 3 studies during the first trimester (12%), in 18 studies during the second trimester (75%), and in 3 studies during the third trimester (12%) (Fig. 3).
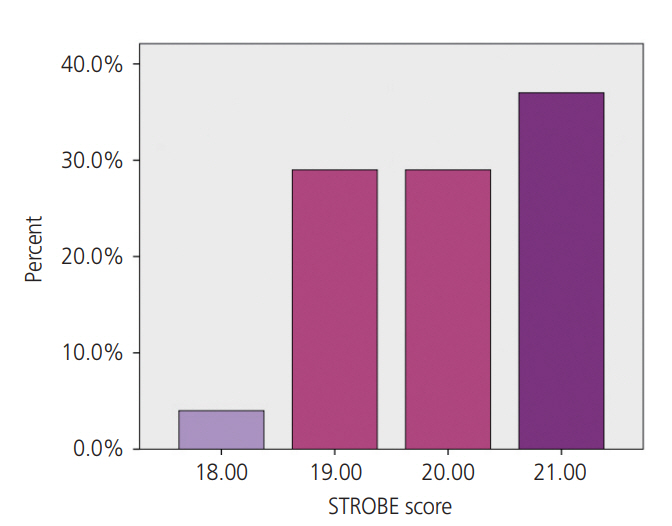
Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) score of different studies.
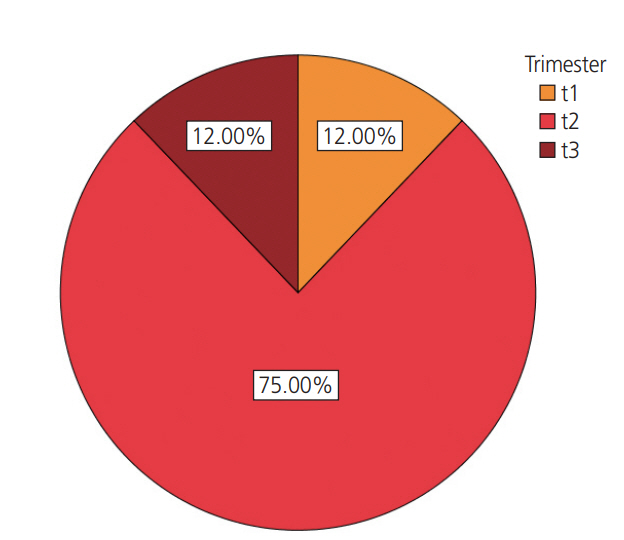
Trimester in which the interleukin-6 test was performed.
The characteristics of the selected studies are listed in Table 2. These studies were conducted in different countries, including China (6), Turkey (4), US (2), Poland (2), India (2), Australia (1), Brazil (1), Prague (1), Tunisia (1), Saudi Arabia (1), Canada (1), Finland (1), and Greece (1). Moreover, for the diagnosis of GDM, 5 studies used the guidelines of Carpenter and Coustan, 1 study used the Indian criteria, 2 studies used the guidelines of International Association of Diabetes and Pregnancy Study Groups (IADPSG), 5 studies used the American Diabetes Association (ADA) guidelines, 4 studies used the National Diabetes Data Group guidelines, 2 studies used the China Diabetes Association Diabetes Branch guidelines, 1 study used the Australasian Diabetes in Pregnancy Society guidelines, 1 study used the Polish Diabetes Association guidelines, 1 study used the American College of Obstetricians and Gynecologists (ACOG) guidelines, 1 study used the Canadian Diabetes Association guidelines, 1 study used the WHO guidelines, 1 study used the Endocrine Society Clinical Practice Guideline/ACOG guidelines, 1 study used the ACOG/ADA guidelines, and 1 study used the Carpenter and Coustan/ADA guidelines. The majority of the studies measured IL-6 levels using the enzyme-linked immunosorbent assay (18), while the others employed multiplex immunoassay (4) or chemiluminescent immunoassay (2).

Results from a systematic review of studies
Fig. 4 shows the significance level of the selected studies. As shown in this diagram, 16 studies exhibited a significant relationship between the serum level of IL-6 and GDM. Therefore, we can conclude that the serum IL-6 level may act as a suitable diagnostic marker for GDM.
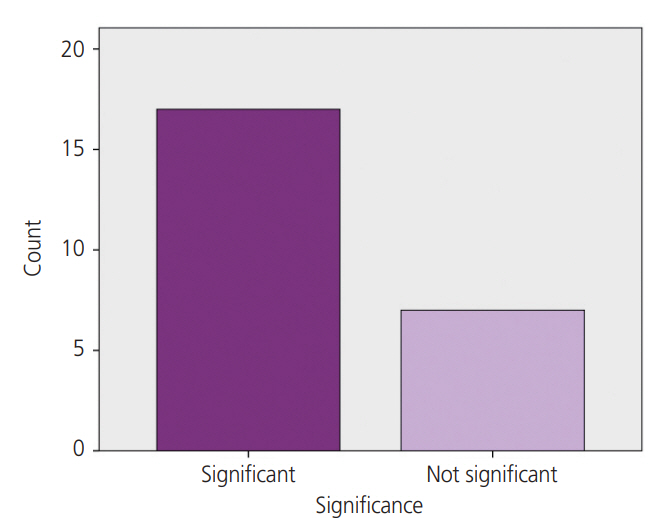
Assessing the significance level of different studies.
Discussion
In the present systematic review, 24 articles were reviewed, most of which demonstrated a significant relationship between IL-6 levels and GDM. Thus, we concluded that IL-6 can be used as a marker to predict the occurrence of gestational diabetes.
Accurate and early diagnosis of women at a high risk of developing GDM provides an opportunity to manage the prenatal care models and apply future interventions to reduce the progression of gestational diabetes, and thereby its associated health care expenses and side effects [40]. However, the diagnostic criteria for GDM is still debatable. A previous study reported a linear relationship between maternal blood glucose levels and adverse perinatal outcomes [41]. The IADPSG recommends that the studies aimed to diagnose gestational diabetes must develop simpler, more cost-effective methods that do not require OGTT [42]. In recent years, there has been a great interest in identifying the role of inflammation during the development of GDM. Inflammatory factors can act as insulin antagonists and cause insulin resistance [43]. IL-6, as a cytokine, plays a crucial role in the pathophysiology of glucose intolerance and serves as a potential serum marker for early screening of glucose intolerance [43].
In type 2 diabetes, inflammatory cytokines may induce insulin resistance by suppressing multiple pathways in target tissues that are responsible for proper insulin signaling [44]. Insulin resistance is associated with abnormal secretion of proinflammatory cytokines, such as IL-6 [4]. In non-pregnant women, BMI and high body fat mass have been found to be associated with elevated levels of serum IL-6 [13]. IL-6 is also secreted by the placenta during pregnancy, which can lead to a chronic inflammatory process in adipose tissue and further assist the development of pregnancy-induced insulin resistance [45]. In GDM, similar to type 2 diabetes, insulin resistance is implicated in the pathophysiology [46]. Type 2 diabetes is considered a chronic inflammatory disease and IL-6 is a risk factor for the development of type 2 diabetes. Therefore, due to similar mechanisms underlying the onset of GDM and type 2 diabetes, IL-6 might act as an effective marker in predicting GDM.
In this systematic review, quantitative analysis of available data on the relationship between serum IL-6 levels and GDM was performed based on 24 selected articles, of which 16 articles showed an association between elevated serum IL-6 levels in women and GDM. For example, the results of a case-control study conducted by Siddiqui et al. [13] that aimed to investigate the association of IL-6 and C-reactive protein with GDM in Indian women demonstrated that the serum levels of IL-6 in women with GDM was significantly higher than in control women. Moreover, IL-6 levels were also associated with pre-pregnancy BMI, fasting blood sugar, and postprandial blood sugar . A study conducted by Yu et al. [22], which aimed at investigating the changes in gut flora and various inflammatory factors in patients with GDM, showed that the serum levels of inflammatory factors, including IL-6, were significantly higher in the case group than that in the control group; moreover, patients with GDM were highly susceptible to intestinal flora imbalances with elevated inflammatory factors, which affected the immune function in these patients and may play an important role in the development of diabetes. Furthermore, the findings of the study conducted by Zhao et al. [23], which aimed to examine the possible association of inflammatory markers with glucose intolerance and GDM in Chinese women, indicated that IL-6 levels were significantly higher in pregnant women with GDM or glucose intolerance compared to those in the healthy control group, and that there was a positive relationship between inflammatory cytokines, BMI, and HbA1c . In the study conducted by Zhang et al. [25], aimed at investigating the association between inflammatory and metabolic biomarkers in women with GDM in Mongolia, showed that the levels of inflammatory and placental biomarkers, including IL-6, in both serum and placenta showed a significant difference between women with GDM and those with healthy pregnancies.
The present review also included studies that did not show a correlation between the serum levels of IL-6 and GDM, such as the study conducted by Abell et al. [24], which aimed at evaluating the relationship between GDM risk using fasting glucose and serum biomarkers at the early pregnancy, and indicated that the serum IL-6 levels did not improve the ability to predict the risk of GDM. The results of another study conducted by Gümüş et al. [29] aimed to evaluate the possible association between clinical and biochemical parameters with GDM and gingivitis; this study showed that there was no association between the serum IL-6 levels and GDM. Similar results were obtained in an another study conducted by Özyer et al. [34] that aimed at investigating the association of inflammatory mediators, including IL-6, with glycemic status in pregnancy; the results of this study indicated that the maternal serum levels of inflammatory mediators are not relevant for assessing GDM during the late second or early trimester. The reason for such differences in the results of these studies can be attributed to the use of different methods and kits for measuring IL-6 levels and dissimilar diagnostic criteria for GDM. Also, the effects of confounding variables on serum IL-6 levels and GDM were not considered in all of the selected articles.
Increased IL-6 secretion during pregnancy has been associated with GDM in several studies. Conversely, OGTT testing with 75 grams of oral glucose, which is currently the gold standard test, is performed almost late in pregnancy and requires overnight fasting. Moreover, consumption of glucose is not very pleasant for a pregnant woman and it requires the collection of blood samples 3 times during the process. However, assessing IL-6 levels does not have the above-mentioned challenges and it is easy, affordable, and tolerable for a pregnant woman. Therefore, IL-6 can be used as a marker for assessing the risk of GDM in pregnant women. Considering the increasing prevalence of gestational diabetes worldwide and the need for timely diagnosis and treatment of GDM to reduce adverse maternal and fetal complications, an acceptable marker such as IL-6 is urgently needed.
Conclusion
The results of this study indicate that serum IL-6 levels are significantly higher in pregnant women with GDM than in healthy pregnant women. Therefore, the evaluation of this marker as an acceptable, inexpensive, and readily available diagnostic criterion for assessing the risk of GDM can be investigated.
One of the limitations of this systematic review is the heterogeneity of the diagnostic criteria for GDM. Different commercial kits and assays have been employed to measure the serum IL-6 levels. Conversely, based on the extensive research and use of multiple studies with different ethnicities, it is difficult to control the effect of this variable. Additionally, all the previous studies that were considered did not offer adequate clinical information for performing a robust meta-analysis.
Acknowledgements
We would like to thank Alborz University of Medical Sciences.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Ethical approval This study has a code of ethics No. IR.ABZUMS.REC.1398.218 approved by Alborz University of Medical Sciences.
Patient consent There is no need for patient consent in this review article.