




Introduction
The most severe form of autosomal recessive congenital ichthyosis is harlequin ichthyosis (HI) [1]. HI is a rare congenital disorder that carries a very high perinatal mortality. Neonates with HI usually do not survive beyond the first few days of life. Ichthyoses are a group of disorders characterized by whitish or dark brown scales on the skin of almost the entire body [2]. The tightness of the skin pulls the area around the eyes and the mouth, forcing the eyelids and lips to turn inside out, and exposing the red inner linings. Moreover, the chest and abdomen of the infant may be severely restricted, making breathing and eating difficult. Globally, the newborn appears to be encased in a tight, parchment-like membrane. The clinical features at birth include eclabium, ectropion, dense plate-like scales covering the entire body, an absent/flat nose, and flattened ears. Flexion contractures of the limbs are also frequently observed [3]. The hands and feet may be hypoplastic and partially flexed. The disease primarily affects the skin; however, other systems can be compromised significantly due to hyperkeratosis and tight armor-like scales which may restrict respiration. Neonates are typically born prematurely, and males and females are affected equally. In patients with a family history, HI is diagnosed by fetal skin biopsy. In addition to ultrasonography, DNA analyses from amniocentesis and chorionic villus sampling (CVS) have also been used for the diagnosis of this rare disorder [4].
Case report
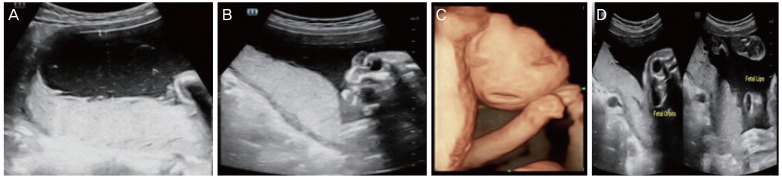
A 30-year-old woman (gravida 3, para 2, D1, L1) presented in the second trimester at 24 weeks gestation for a routine antenatal checkup. The patient had one infant previously that was affected by HI. In the present pregnancy, a fetal anomaly scan was performed using a 3.5 MHz linear transducer on an Esaote machine. Two-dimensional (2D) and 3D sonographic examinations were performed. The examinations revealed a single live intrauterine gestation in breech presentation, and no significant abnormalities were detected at this time. In view of the patient's prior history, an ultrasound with 3D and 4D real-time sonography was performed at 28 weeks. At this examination, the fetus was still in breech presentation, and there was polyhydramnios with internal echoes in the amniotic fluid (Fig. 1A). Intrauterine growth restriction was evident. The fetal face showed hypoechoic masses located anterior to each orbit (Fig. 1B). The fetus showed a flat facial profile with an absent nose (Fig. 1C), a large, gaping, wide open mouth (Fig. 1D), and a dysplastic ear (Fig. 2A). The fetal limbs showed mild flexion deformities with restricted movements. The toes appeared to be short, and the fingers were held in fixed flexion (Fig. 2B). Physicians counseled the parents about the fetus's poor prognosis and complications. A spontaneous vaginal delivery occurred at 32 weeks, and the baby died after 12 hours. At birth, the infant showed characteristics typical of HI. These included ectropion (complete eversion of eyelids with occlusion of eyes), eclabium (eversion of the lips), and thickened and fissured skin. Flexion deformity of all joints of the limbs was noted (Fig. 2C). As this is an autosomal recessive condition, the parents were advised to participate in fetal blood sampling for DNA banking and mutation analysis of the adenosine triphosphate-binding cassette transporter protein A12 (ABCA12) gene, and to consent to having a skin biopsy for histopathological examination. However, the parents declined to participate due to financial constraints. A family and medical history revealed consanguinity, but there was no history of HI cases in previous generations.
Fig. 1
(A) Polyhydramnios with echogenic internal echoes. (B) Edematous eyelids. (C) Three-dimensional image showing ectropion and eclabium and fixed and hyperflexed fingers which are typical features of HI. (D) Fetal face showing characteristic features of ichthyosis. Left: protruding eyes; right: showing open mouth with thick lips.

Discussion
Congenital ichthyoses can be divided into 3 subtypes: lamellar ichthyosis, nonbullous congenital ichthyosiform erythroderma, and HI [5]. HI is the most severe form of congenital ichthyosis. The first description of HI was made in 1750 by Reverend Oliver Hart, and the first case of antenatal diagnosis was reported in 1983 [6]. The overall incidence of HI is 1 in 300,000 births [7,8]. HI is a congenital epidermal disorder that shows abnormal and diffuse hyperkeratosis and loss of the protective skin barrier. In humans, normal cornification of the skin begins between 14 and 16 weeks of gestation. The ABCA12 gene is essential for providing instructions on how to make a protein that is required for normal skin cell development. This protein plays an important role in the transport of lipids in the epidermis. Mutations in ABCA12 gene prevent the cell from making the ABCA12 protein. A loss of function in the ABCA12 protein disrupts the normal development of the epidermis. This subsequently results in extreme thickening of the keratin layer of the skin and the formation of hard scales [9]. Most of affected neonates die within hours or days after birth due to sepsis, electrolyte imbalance, or mechanical restriction of breathing [10] secondary to restricted chest expansion and prematurity. Thickened, cracked skin leads to impaired temperature regulation and increased risk of infection. The most common sonographic features observed in HI are a large open mouth, a flat nose, ectropion, short feet, and abnormal limb position. Intrauterine growth restriction, polyhydramnios/oligohydramnios, increased echogenicity of amniotic fluid, and floating membranes may also be associated with HI. Because eclabium and ectropion manifest in the third trimester, a diagnosis of HI based solely on these findings occurs too late. However, achieving an early sonographic diagnosis of HI is difficult. Short feet may be an early marker for HI, especially in families with a history of siblings affected by HI [11,12]. The other early feature is fixed, extremely hyperflexed toes, as described in a study by Vijayaraghavan et al. [13]. A literature review found that the earliest diagnosis by 3D occurred at 22 weeks in cases with a previous history, whereas in unsuspected cases the earliest diagnosis was made at 30 weeks [14]. Differential diagnoses include arthrogryposis, aplasia cutis, Gaucher disease (collodion baby), Sjogren-Larsson syndrome, Conradi-Hunermann-Happle syndrome, Neu Laxova syndrome, and trichothiodystrophy [15]. HI is an autosomal recessive condition, and parents who have already had an affected child have a 25% risk of recurrence in each pregnancy [16]. Consequently, the high recurrence rate allows a prenatal diagnosis to be performed for families at risk. HI can be diagnosed using either amniocentesis or CVS. Both of these procedures are used to obtain a DNA sample from the fetus to look for mutations in the ABCA12 gene. However, ultrasonography can also diagnose HI, and this is particularly important as it allows antenatal diagnosis even in cases with no family history of the disease. Early sonographic diagnosis is difficult, and most of cases are diagnosed in the third trimester. Hence, prenatal ultrasonography can establish the diagnosis of HI in the early third trimester.
HI is a rare autosomal recessive disorder with high subsequent recurrence. DNA analysis for ABCA12 mutations can be offered to suspected cases and to families who have previously been affected. The prenatal ultrasonography findings suggestive of a harlequin fetus are atypical facial dysmorphism, a large open mouth, the absence of typical nasal morphology, partitioned cystic formations in front of the eyes, the absence of typical ear morphology, thick skin, minimal fetal movement with stiff limbs in a semi-flexed position, limb anomalies with hypoplastic fingers, toes, and short phalanges, clubfoot, shriveled hands that do not open, hyperechogenic amniotic fluid, and an absence of associated visceral anomalies. 3D imaging is essential for understanding the 2D images and enabling diagnosis of HI. The characteristic features in prenatal ultrasonography tend to appear late, so scans should be repeated even when the second trimester anatomy scan is normal. In addition, these scans can help in situations when a DNA diagnosis is unavailable.






")











