Posterior reversible encephalopathy syndrome in a woman who used gonadotropin-releasing hormone agonists: a case report
Article information

Abstract
Posterior reversible encephalopathy syndrome (PRES) is a newly described adverse effect possibly associated with gonadotropin-releasing hormone (GnRH) agonist therapy. We report a case of PRES after 2 doses of depot GnRH agonists in a 44-year-old woman with a huge myoma uteri and iron-deficiency anemia. Brain magnetic resonance imaging showed high signal lesions in both occipital lobes on fluid-attenuated inversion-recovery (FLAIR) images, compatible with PRES. After treatment with anticonvulsant, she recovered both radiographically and clinically. The association between PRES and GnRH agonist use is still enigmatic, and thus should be further clarified.
Introduction
Gonadotropin-releasing hormone (GnRH) agonists have been widely used to treat estrogen-dependent benign gynecologic conditions such as endometriosis, adenomyosis, and uterine leiomyomas [1]. Common adverse effects of GnRH agonists include hot flashes, unstable mood, headaches, and trouble sleeping [2]. It has been suggested that GnRH agonist use is associated with catamenial seizures [3] and ischemic heart disease [4].
Posterior reversible encephalopathy syndrome (PRES) refers to a disorder of reversible subcortical vasogenic brain edema causing acute neurological symptoms such as seizures, encephalopathy, headache, and visual disturbances. Brain imaging predominantly reveals vasogenic edema involving the bilateral parieto-occipital regions [5]. PRES is generally reversible, both radiographically and clinically, and has a favorable prognosis [6].
This syndrome is associated with renal failure, blood pressure fluctuations, cytotoxic drug intake, autoimmune disorders, and pre-eclampsia or eclampsia [56]. Cytomegalovirus or bacterial infection in patients with rejected transplants are also etiologic factors [5]. Two recent case reports suggest that GnRH agonists use is associated with PRES [78]. To date, it is not well known whether GnRH agonists induce PRES.
Here we report a case of PRES in a woman with huge myoma uteri who received two doses of depot GnRH agonists.
Case report
A 44-year-old parous woman visited the Department of Gynecology in our hospital. She had a huge myoma uteri (largest diameter 12 cm) and severe iron-deficiency anemia (blood hemoglobin 4.3 g/dL) (December 27, 2016). She received a single dose of intravenous iron at a private clinic and took oral iron regularly.
In our hospital, she was subcutaneously treated with 2 doses of 3.75 mg depot leuprolide acetate (leuprorelin; Leuplin DPS, Takeda, Japan) 4 weeks apart (January 10, 2017 and February 10, 2017).
Seventeen days after the second dose of leuprolide acetate (February 27, 2017), she visited the emergency room in our hospital due to aggravated headache and dizziness, which began 7 days prior. Her blood pressure was 140/86 mmHg, pulse rate was 79/min, respiratory rate was 26/min, and body temperature was 36.0°C. Her headache encompassed the entire head and included eyeball pain. When the head was suddenly forced to the right, the eyeball also deviated to the right and generalized tonic-clonic seizure occurred simultaneously. She was a nonsmoker and did not drink alcohol.
Serologic tests revealed no abnormalities, and blood hemoglobin was 13.6 g/dL. Electrocardiogram showed normal findings, and her computed tomography scan revealed neither focal lesions nor intracranial hemorrhage in the brain. Her brain magnetic resonance imaging (MRI), however, showed multiple lesions with high signal intensity in both occipital lobes on fluid-attenuated inversion-recovery (FLAIR) image, mainly involving the cortex (Fig. 1). These MRI findings were compatible with PRES. Electroencephalogram and cerebrospinal fluid analysis was within the normal range. After hospitalization, an anticonvulsant (levetiracetam; Keppra, UCB Pharmaceuticals, Brussels, Belgium) was administered. She gradually recovered from the headache and was discharged after 3 days. Four weeks later, her brain MRI showed a remarkably improved occipital lesion (Fig. 2). Thereafter, the anticonvulsant was gradually tapered and was stopped 1 week later.
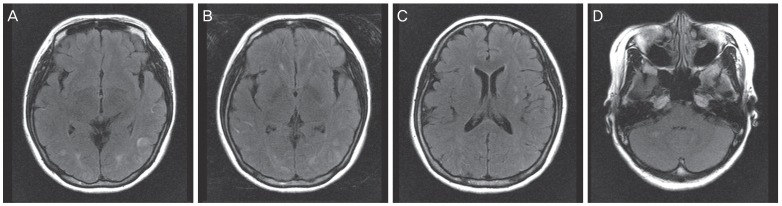
Initial brain magnetic resonance imaging shows the abnormal high signal change in both occipital lobe on fluid-attenuated inversion-recovery (FLAIR) image (A, B), left putamen (C), and right cerebellum (D).
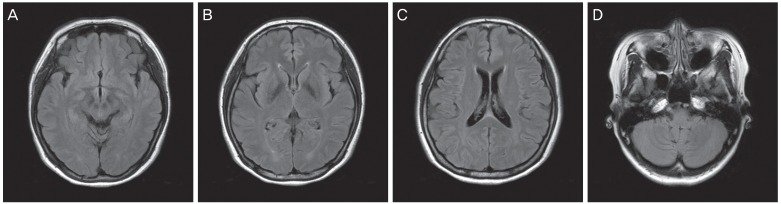
Follow-up brain magnetic resonance imaging at 4 weeks after the initial visit demonstrates that the original lesions of high signal intensity in both occipital lobe (A, B), left putamen (C), and right cerebellum have disappeared (D).
Discussion
The pathophysiology of PRES remains controversial, and two main hypotheses have been suggested; impaired cerebral autoregulation resulting in an increase in cerebral blood flow, and endothelial dysfunction with cerebral hypoperfusion [56]. Under both hypotheses, abnormalities in cerebral blood perfusion may be the key mechanism underlying blood-brain barrier dysfunction and cerebral vasogenic edema [5].
GnRH agonists induce low estrogen status, and in turn, protective effects of estrogen on endothelial cells may be attenuated. Estrogen has been known to have some protective capabilities against ischemia-reperfusion injury in various organs [9]. Ischemic heart disease can occur after GnRH agonist injection [4]. Ischemic heart disease and cerebrovascular accidents share common risk factors, and GnRH agonist-induced hypoestrogenic status might play a role in the development of PRES [8].
Hayashi et al. [7] suggested that the sudden increase in physical activity involved in avoiding a traffic accident may have induced PRES in a woman who received GnRH agonist therapy. They suggested that GnRH agonists induce vasoconstriction, but sudden changes in physical activity that occur during driving may have induced abrupt vasodilation and subsequent impaired cerebral autoregulation as well as blood-brain barrier dysfunction. Lee et al. [8] suggested that, similar to immunosuppressive and cytotoxic drugs, GnRH agonists have direct cytotoxic effects on the vascular endothelium.
Activation of the immune system (especially T lymphocytes) leads to endothelial cell activation and the release of various mediators including histamine, free radicals, nitric oxide, bradykinin, and arachidonic acid [10]. These mediators activate the production of pro-inflammatory cytokines (e.g., tumor necrosis factor-α, interleukin (IL)-1, IL-6, and interferon-γ) [11]. Upregulation of endothelial surface antigens and endothelin release affect local vascular tone [12]. These changes all result in vascular instability, vasoconstriction, and downstream hypoperfusion. Blood-brain barrier dysfunction may also lead to vasogenic cerebral edema [13]. The association of PRES with various autoimmune diseases, infection, and sepsis has been noticed [5], and when PRES symptoms are present, these conditions should be ruled out.
The concept of GnRH agonist-related PRES itself is still unclear. However, in our patient, there was no underlying hypertension or kidney disease, and she did not take cytotoxic or immunosuppressive drugs. There was no evidence of infection or sepsis. MRI showed characteristic lesions compatible with PRES, thus brain tumors and cerebral infarction could be ruled out. In such a condition where a woman develops PRES after 1 or 2 GnRH agonist doses, GnRH agonist-related PRES should be considered.
PRES might be associated with rapid correction of severe iron-deficiency anemia. Indeed, hemoglobin levels were normalized within two months in this case (from 4.3 to 13.6 g/dL). Rapid correction of severe anemia might result in increased blood viscosity, which could induce cerebral hypoperfusion, blood-brain barrier dysfunction, and vasogenic cerebral edema [7]. GnRH agonists are usually administered for induction of amenorrhea as well as correction of severe iron-deficiency in women with large fibroids. It may therefore be difficult to deduce whether the PRES was induced by rapid correction of severe iron-deficiency or GnRH agonist use.
In two former case reports, as in our case, PRES occurred after leuprolide injection [78]. It is currently unknown whether other GnRH agonists are associated with PRES, however spontaneous seizure has been reported to occur after leuprolide, goserelin, or naferelin use [3].
There is no specific treatment for PRES, but the disorder is usually reversible when the precipitating cause is eliminated or treated [5]. Seizures can be treated with antiepileptic drugs, but targeted antiepileptic drugs are not available [5]. It has been suggested that treatment of hypertension is important, although no studies measuring the effect of hypertension control on PRES resolution have been conducted [5]. The prognosis of PRES is usually favorable, and most patients recover completely [5]. One report notes the mean time to full clinical recovery to be between 2–8 days [14], however, some patients take several weeks to achieve full recovery [5].
The association between PRES and GnRH agonist use is still enigmatic, and should thus be further clarified.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.
Ethical approval: The study was approved by the Institutional Review Board of Seoul National University Bundang hospital (IRB No. B-1812-511-701) and performed in accordance with the principles of the Declaration of Helsinki.