Prevalence of folic acid supplement consumption before and during pregnancy, and its determinants among community health center referrals
Article information

Abstract
Objective
The aim of this study is to assess the prevalence and determinants of folic acid supplementation among women referred to community health centers.
Methods
This was a cross-sectional study conducted in 325 women referred to community health centers. The subjects were selected from 8 community health centers, using a stratified sampling technique. Data regarding demographics, socioeconomic status, obstetrics, folic acid supplementation status, and household food security status were obtained via questionnaires. The data was analyzed in SPSS v22.
Results
The prevalence of folic acid supplementation both before and during pregnancy was 54.5%. The results of the study showed that folic acid supplementation had a significant positive association with education level (odds ratio [OR],0 .441; 95% confidence interval [CI], 0.199–0.977; P<0.05), being employed (OR, 0.353; 95% CI, 0.148–0.840; P<0.05), and planned pregnancy (OR, 18.113; 95% CI, 7.371–44.51; P<0.001). However, other variables, including age, husband's age, husband's education and employment status, the number of prior pregnancies, economic satisfaction, and household food security, were nonsignificant factors affecting folic acid supplementation.
Conclusion
Women with lower socioeconomic status are less likely to take folic acid supplements, and more effort should be made to increase their awareness of the importance of supplementation. Unplanned pregnancy is another strong risk factor for not supplementing with folic acid, and thus should be avoided.
Introduction
Nutritional status plays an important role in the critical period of pregnancy for women and their unborn infants [1]. Pregnant women need more folic acid for the growth and development of the fetus [2]. Folic acid deficiency during pregnancy may lead to health problems in mothers, such as anemia and peripheral neuropathy, and in infants, including congenital abnormalities [2] and neural tube defects (NTDs) [3]. There are various risk factors for NTDs including poor maternal nutritional status and maternal folate deficiency during pregnancy [4]. Supplementation with folic acid has, therefore, been identified as a factor in decreasing NTDs in infants [5678910]. Implemented as a worldwide policy by the World Health Organization (WHO) in 2006, the daily consumption of 400 µg of a folic acid supplement is recommended for women of childbearing age who are planning a pregnancy [11]. Nevertheless, the implementation of this recommendation remains inadequate [12]. The results of studies have shown that the prevalence of folic acid supplementation is often insufficient in the preconception period [1314]. Several factors have been associated with preconception folic acid supplementation, including maternal age [12]; educational status [13]; marital status [1]; employment status [15]; the number of prior pregnancies [12]; income [16]; whether the pregnancy was planned or unplanned [13]; smoking status [17]; and the level of knowledge, attitude, and awareness of the importance of folic acid supplementation before and during pregnancy [1417]. It is necessary to identify the determinants of folic acid supplementation before and during pregnancy in order to increase the prevalence of folic acid supplementation, and thus decrease the negative consequences of folic acid deficiency on maternal and infant health. This study, therefore, aimed to assess the prevalence and determinants of folic acid supplementation before and during pregnancy, among women referred to community health centers in the city of Tehran.
Materials and methods
This cross-sectional study was carried out in 325 women who had given birth and had been referred to community health centers in western Tehran between March and June 2014.
Subjects were selected from 8 community health centers across 16 areas, using a stratified sampling technique (with each center as a stratum). These selected centers provided suitable distributions of the population and geographic area). The sample size for each stratum was proportional to population size, and the convenience sampling method was used to select the samples within a center.
Information regarding demographics (age of women and their husbands), socioeconomic status (education level, occupational status, and economic satisfaction score), obstetrics (planned or unplanned pregnancy and the number of prior pregnancies), folic acid supplementation before and during pregnancy, and household food security status was collected via questionnaires. In order to assess the economic satisfaction score, mothers were asked to select a score from 1 to 10 (subjectively) to indicate their satisfaction with their household economic status.
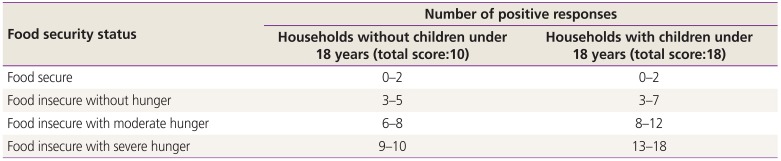
The 18-item US Department of Agriculture (USDA) questionnaire [18] was used for assessing household food security status. The questionnaire was completed by interviewing participants, and was scored by the researchers as follows: responses “most of the time correct” and “sometimes correct” to questions 1 to 3 and 11 to 13; “almost every month” and “some months” to questions 5, 10, and 16; and “yes” to questions 4, 6 to 9, 14, 15, 17, and 18 were scored 1; and responses “is not correct,” “does not know or avoids,” “only once or twice a month,” and “no” were scored 0. The total score was calculated based the number of positive responses, and women were subsequently divided into 4 groups based on the scores: (a) food secure, (b) food insecure without hunger, (c) food insecure with moderate hunger, and (d) food insecure with severe hunger (Table 1) [19]. In order to analyze the data, groups (c) and (d) were combined to compose the food insecure with hunger group. The validity of this questionnaire and its applicability has been previously demonstrated [20].

Classification of the Household food security status based on scores
The data were analyzed in SPSS version 22 (IBM Inc., Chicago, IL, USA). Associations of folic acid supplementation (both before and during pregnancy) with quantitative variables were assessed using logistic regression, and associations with qualitative variables were assessed using the χ2 test. Finally, all variables were assessed in a logistic regression model to determine predictors of folic acid supplementation among women. A value of P<0.05 was considered significant.
Results
In this study, the majority of women were homemakers (86.5%), had earned a high-school diploma or higher (78.2%), were food secure (65.8%), and had a planned pregnancy (79.4%) (Table 2). The results showed that 182 (56%) and 302 (92.9%) of the women had taken folic acid supplements before and during pregnancy respectively (for at least 1 month). However, only 177 (54.5%) of the women had taken folic acid supplements before pregnancy and continued to supplement during pregnancy (for at least 1 month). The associations between supplementation and the age of the woman, and between supplementation and the age of the husband, were assessed via logistic regression, and these results were not statistically significant (Table 3). The results also did not show any significant association between economic satisfaction scores and folic acid supplementation (Table 3). Logistic regression showed a significant association between the number of prior pregnancies and supplementation status (odds ratio, 0.781; confidence interval, 0.617–0.989; P<0.05) (Table 3).

The association of folic acid supplementation with qualitative variables

The association of folic acid supplementation with quantitative variables
With the χ2 test, the education levels of the women who had taken supplements, and the education levels of their husbands, were found to be significantly higher (P<0.001) (Table 2). Unplanned pregnancy was another strong predictor of folic acid supplementation (P<0.001) (Table 2). The husband's employment status did not play an important role in supplementation status (Table 2). However, the ratio of homemakers to employed women who had taken folic acid supplements was lower (P<0.05) (Table 2). In the current study, household food security status was also assessed in both groups. The χ2 test showed a significant decrease in supplementation with increasing levels of food insecurity (P<0.05) (Table 2).
In logistic regression, after adjustment for variables, only the education (P<0.05) and employment (P<0.05) status of women, along with unplanned pregnancy (P<0.001), were recognized as significant predictors of supplementation status (Table 4).

Final logistic regression model for the predictors of folic acid supplementation
Discussion
In this study, the factors affecting folic acid supplementation before and during pregnancy were assessed among women referred to community health centers. Lower education levels (of women), being a homemaker, and unplanned pregnancy were the significant factors associated with the lower supplementation of folic acid, both before and during pregnancy.
The prevalence of women who had taken folic acid supplements for at least 1 month before pregnancy, and continued to supplement into pregnancy, was 54.5%. In a study conducted by Riazi and colleagues [21] in Hamadan, only about 9.6% of women consumed folic acid supplements before pregnancy, which was less than what was seen in the current study. In a study by Nosrat et al. [22], 20.12% of women in Golestan province consumed folic acid supplements during the preconception period. Mashayekhi et al. [14] also reported that about 25.07% of women in Tabriz consumed folic acid supplements for at least 1 month before pregnancy, and 34.82% supplemented with folic acid during the first trimester. In a survey of Italian women, De Santis et al. [13] found that 43.4% of participants took folic acid before becoming pregnant. In the current study, the prevalence of women consuming folic acid supplements was higher before (56%) and during (92.9%) pregnancy than in other studies. Although the women's awareness about the importance of consuming folic acid supplements was not directly assessed in the current study, such large differences may indicate an increasing trend in female awareness and knowledge about the importance of folic acid supplementation and its impact on infant health. The difference in geographic areas may be another reason for the large inconsistencies observed.
Socioeconomic status, including women's education level and employment status, were significant determinants of folic acid supplementation. This means that the prevalence of folic acid supplementation was statistically higher in women with higher education levels and who were employed. These findings are consistent with studies by Riazi et al. [21], Roth et al. [15], and De Santis et al. [13]. It has been shown that higher education levels in women can increase their awareness about the necessity of folic acid supplementation, and their understanding of the important period of folic acid supplementation [1423].
In the current study, economic satisfaction status was assessed subjectively in order to evaluate household economic status, because the participants may have wished to avoid declaring their actual incomes. The results showed higher scores for economic satisfaction in women who consumed folic acid supplements, but this was not statistically significant. In a study conducted by Tamim et al. [17], better economic status was associated with folic acid supplementation. In Iran, community health centers are well distributed across the urban and rural areas of the country in order to provide primary health services for the population. Supplements including iron and folic acid are freely distributed to pregnant women [14], so this may be one reason for the lack of a significant difference in supplementation between women of different economic status.
Food insecurity was another variable evaluated in this study. According to the USDA, food insecurity is defined as, “a household-level economic and social condition of limited or uncertain access to adequate food” [24]. Food insecurity affects dietary quality and quantity of food intake [25]. In a study conducted by Davison et al. [26], food insecurity was associated with poor dietary quality and suboptimal intakes of folate. Since many food-insecure women are undernourished, strategies such as micronutrient supplementation or fortification can be used in order to improve nutritional status [27]. The results of this study showed a decreasing trend in supplementation with increased levels of food insecurity, but this correlation was not found to be statistically significant in logistic regression. This nonsignificant association between food insecurity and supplementation may be due to the free distribution of supplements in community health centers in Iran, as mentioned above. However, food insecure households still need more attention and support.
Although planned pregnancy does not necessarily lead to folic acid supplementation [28], unplanned pregnancy is one of the most important reasons for the lack of folic acid supplementation before pregnancy [1629]. The results of the current study recognized unplanned pregnancy as a robust risk factor affecting supplementation. This finding is consistent with studies by De Santis et al. [13] and Roth et al. [15]. However, planned or unplanned pregnancy was not found to be a significant factor in supplementation among Ethiopian women [30]; which may have been related to low female awareness about the importance of folic acid, lower prescription levels of folic acid, and less education from healthcare providers.
In the current study, the number of prior pregnancies was higher in women who did not use folic acid supplements, but this relationship was not statistically significant. In the study conducted by Dessie et al. [30] of pregnant women in Ethiopia, the number of pregnancies was not an important factor affecting the consumption of folic acid supplements. This finding is also consistent with Rasmussen and Clemmensen's study [23]. On the one hand, in a study conducted by Vitale et al. [16], the number of pregnancies was a negative predictor for supplementation with folic acid, while on the other hand, in a study of Lebanese women by Nasr Hage et al. [12], folic acid intake was significantly associated with a higher number of pregnancies. Based on the different studies, an inconsistency is observed about the association between the number of prior pregnancies and folic acid supplementation. Perhaps this association varies based on the particular contexts of each study.
Finally, it should be noted that although there was no significant relationship between folic acid supplementation with some variables, we cannot report the lack of association with certainty, as this could be due to the limited sample size.
In the current study, the knowledge, attitude, and awareness of women regarding the importance of consuming folic acid supplements before and during pregnancy, as well as the subsequent consequences to mothers and infants due to not supplementing with folic acid, were not assessed. Future studies with larger sample sizes are recommended to evaluate these factors, and to investigate the impact of folic acid supplementation on birth outcomes.
The current study assessed the prevalence of and factors affecting folic acid supplementation before and during pregnancy, among women referred to community health centers. The results of the study showed that slightly more than half (56%) of women had taken supplements before pregnancy. Although most women consumed the supplements during pregnancy, because of the importance of having a sufficient folate status before pregnancy, it is essential that supplementation is started before pregnancy, not after pregnancy is confirmed. In this study, several factors affecting supplementation were identified. Lower education levels of women, being a homemaker, and unplanned pregnancy were the significant factors associated with lower supplementation of folic acid both before and during the pregnancy period. Given that women with lower socioeconomic status are more vulnerable to a lack of folic acid supplementation, more efforts should be made to increase the knowledge, attitude, and awareness of women about the importance of supplementation, and the consequences of insufficient supplementation, by community health service staff and the media. Planned pregnancy is another strong factor influencing supplementation. Unplanned pregnancy should therefore be avoided by adopting appropriate policy makers’ strategies, including increased education by health center staff and the media.
Acknowledgements
The authors would like to thank the staff of the community health centers and the women who participated in the study for their kind cooperation.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.
Ethical approval: The protocol was approved by the Research Council and Ethical Committee of Qazvin University of Medical Sciences, No. D.44.21039. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Patient consent: All participants gave their informed consent to participate in the study.