Total and ionized serum magnesium and calcium levels during magnesium sulfate administration for preterm labor
Article information

Abstract
Objective
This study aimed to estimate the association between total and ionized magnesium, and the changes in serum magnesium and calcium levels in patients with preterm labor during magnesium sulfate (MgSO4) administration.
Methods
The study population included 64 women who were candidates for intravenous MgSO4 treatment for preterm labor. Serial blood samples were taken and measured total magnesium (T-Mg), ionized magnesium (I-Mg), total calcium (T-Ca), and ionized calcium (I-Ca) levels every one-week interval (1st, 2nd, 3rd).
Results
There was no significant difference in T-Mg and I-Mg levels during MgSO4 administration (P>0.05). There was no significant difference in T-Ca and I-Ca levels during MgSO4 administration (P>0.05). Compared before and after administration of MgSO4, T-Mg and I-Mg levels and T-Ca levels were changed allow statistically significant (P<0.05). But, there was no significant difference in the I-Ca serum levels before and after MgSO4 administration (P=0.495). The I-Mg levels for patients with adverse effect were higher than other group but did not reach statistical significance (P>0.05). There was significant correlation between levels of I-Mg and T-Mg (I-Mg=0.395×T-Mg+0.144, P<0.01).
Conclusion
There were no significant differences in serum Mg and Ca levels during MgSO4 administration for preterm labor. Compared to the before and after administration of MgSO4, only I-Ca levels were not substantially changed. There are significant correlations between I-Mg and T-Mg levels during administration of MgSO4 and I-Mg level seemed to have more correlation with adverse effect than T-Mg.
Introduction
Intravenous magnesium sulfate (MgSO4) is widely used in perinatal medicine to treat preterm labor [12]. The ability of MgSO4 to inhibit uterine contractility both in vivo and in vitro has been appreciated for over 40 years. Most recently, administration of MgSO4 to women at risk of preterm delivery has been shown to decrease the probability of cerebral palsy [34]. It is well-known that magnesium (Mg) can be toxic to pregnant women. In general, the therapeutic range of total magnesium (T-Mg) is considered to be 4–8 mg/dL [56]. Patellar reflex disappears if the serum level reaches 8 mEq/L (4.0 mmol/L) due to the noncompetitive antagonism of calcium (Ca) ions by Mg at the neuromuscular junction [7]. Also, respiratory depression is possible when Mg levels reach 12 mEq/L [34]. Furthermore, Mg is transported through the placenta via an active transport mechanism [89], and its administration to the mother may lead to fetal hypermagnesemia and deleterious neonatal consequences [10]. Early case reports suggested that Mg ions given to the mother might induce neuromuscular blockade in neonates and manifest as respiratory depression, hypotonia, and hyporeflexia [1011]. Thus, close monitoring of serum Mg levels is essential.
The therapeutic range for T-Mg, however, it is still being debated. The reason is that ionized magnesium (I-Mg), like ionized calcium (I-Ca), possesses physiological activity in vivo. Mg exists in various form [12]. Of the T-Mg in the body, 67% is found in bone and hard tissue; 31% is found inside cells; and approximately 2% is found in serum. Intracellular T-Mg vastly exceeds extracellular or serum T-Mg levels. In contract, intra- and extracellular I-Mg appear to be comparable [13]. Also, I-Mg passes through the cell membrane relatively quickly, suggesting that the 2 I-Mg reservoirs are in dynamic equilibrium. These observations suggest that extracellular measurement of I-Mg in whole blood, plasma, or serum reflects dynamic intracellular-extracellular Mg homeostasis. In either instance, cardiac and vascular smooth muscle are exposed to the I-Mg concentration present in the blood plasma, and this would be the most likely value to predict a physiological response [1415].
To investigate the stability of long-term use of MgSO4, we tried to estimate the changes in the association between I- and T-Mg levels, and the changes in T-Mg, I-Mg, total calcium (T-Ca), and I-Ca levels in patients with preterm labor during MgSO4 administration.
Materials and methods
The study population included 64 women who were candidates for intravenous MgSO4 treatment for preterm labor at the Maternal Care Center of Chonnam University Hospital from August 2014 to May 2015. The preterm labor was defined as of regular uterine contractions accompanied by a change in cervical dilation, effacement, or both, or initial presentation with regular contractions and cervical dilation of at least 2 cm [16]. Exclusion criteria were contraindications to tocolysis, such as advanced labor, fetal demise, severe pre-eclampsia, lethal fetal anomaly, overt or suspected chorioamnionitis and severe hemorrhage. During the study, first line tocolytic treatment consisted of intravenous MgSO4. The second line included ritodrine, and the third line treatment was atosiban. Patients with preterm labor between 24.0 and 33.6 weeks of pregnancy received glucocorticoids for fetal pulmonary maturation.
MgSO4 was administered at a loading dose of 2 g for 1 hour followed by a maintenance dose of 0.8–3.0 g/hr, which was titrated as the uterine contraction changed. The maximum dose was 3 g/hr. If 3 g/hr MgSO4 did not decrease uterine contractions, other tocolytic agents were used instead. Uterine contractions were regularly monitored with electronic fetal monitoring and chest X-ray was performed to monitor pulmonary edema once a week. The patients were monitored routinely by evaluation of patellar reflexes, respiratory rate and urinary output measurement daily. Furthermore, we investigated the occurrence of facial flushing, headache, nystagmus, nausea, dizziness, dry mouth and lethargy during administration of MgSO4. If absence of contraction (2 or less per 10 minutes) or presence of side effect, MgSO4 was either tapered or discontinued.
Maternal serum T-Mg, I-Mg, T-Ca, and I-Ca levels were measured immediately before MgSO4 therapy, and at 8, 15, and 22 days after beginning the loading dose until administration was discontinued. The blood was obtained by direct puncture to a vein. I-Mg and Ca were analyzed directly from whole blood with an ion-selective electrode (NOVA 8 Analyzer; NOVA Biomedical Corp., Waltham, MA, USA) at the time of the blood draw. The T-Mg and T-Ca levels were measured using a Hitachi 7700 automatic analyzer (Hitachi, Tokyo, Japan).
Results were expressed as mean±standard deviation. The associations between I-Mg and T-Mg, and I-Ca and T-Ca were calculated using Pearson's correlation coefficient test. A P<0.05 was considered significant.
Results
A total of 64 patients with preterm labor were studied. Table 1 shows the clinical characteristics. The average maternal age was 29.7±3.2 years. The mean gestational week at the initiation of MgSO4 administration in patients with preterm labor was 28.0±3.6 weeks. The administration duration was 17.1±11.3 days. The total dose of MgSO4 administration was 787.7±619.8 g.

Clinical characteristics of patients with preterm labor administrated with magnesium sulfate (n=64)
Table 2 shows the results according to MgSO4 administration duration. To investigate the stability of long-term use of MgSO4, the data could be divided into 3 groups — within 7 days (G1), within 14 days (G2), and more than 15 days (G3) of MgSO4 administration duration. The dose of MgSO4 during the last 7 days was 350.91, 301.54, and 332.51 g, for G1, G2, and G3, respectively. There were no significant differences in the total dose of MgSO4 administered among the 3 groups (P=0.634). The average T-Mg and I-Mg levels were 3.46±0.86 (G1) vs. 3.15±0.91 (G2) vs. 3.51±1.08 (G3) mg/dL and 1.74±0.42 (G1) vs. 1.70±0.62 (G2) vs. 1.87±0.56 (G3) mEq/L, respectively. The average T-Ca and I-Ca levels were 7.80±0.48 (G1) vs. 7.82±0.61 (G2) vs. 7.82±0.58 (G3) mg/dL and 2.11±0.16 (G1) vs. 2.10±0.15 (G2) vs. 2.12±0.18 (G3) mEq/L, respectively. There were no significant differences between T-Mg and I-Mg (P=0.540 and P=0.611, respectively) and T-Ca and I-Ca (P=0.993 and P=0.892, respectively) according to MgSO4 administration duration.

Changes in T-Mg and I-Mg and T-Ca and I-Ca blood plasma levels in patients with preterm labor (n=64) administered magnesium sulfate according to administration duration
Fig. 1A shows the results of T-Mg and T-Ca levels between before and after MgSO4 administration. The average baseline (preload) T-Mg and T-Ca level for all patients was 2.09±0.85 and 8.25±0.55 mg/dL. Both T-Mg and T-Ca levels increased after infusion, reaching a statistically significant increase compared to the baseline (T-Mg: P<0.05; T-Ca: P<0.05). In Fig. 1B, the average baseline I-Mg and I-Ca level was 1.34±0.52 and 2.07±0.15 mEq/L. There was a significant difference in the I-Mg serum levels before and after MgSO4 administration (P<0.05). However, there was no significant difference in I-Ca levels before and after MgSO4 administration (P=0.495).
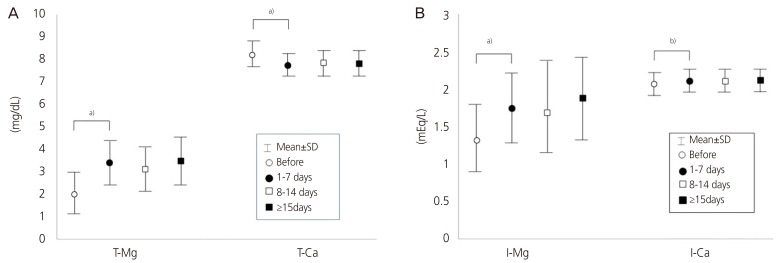
Comparison of total magnesium (T-Mg) and total calcium (T-Ca) levels (A) and ionized magnesium (I-Mg) and ionized calcium (I-Ca) levels (B) in patients with preterm labor between before and after magnesium sulfate administration.
Superscript marks considered statistically significant: a)P<0.05 or b)P>0.05.
Table 3 shows the results of comparing each level (T-Mg and I-Mg, T-Ca and I-Ca), depending on the presence or absence of adverse effects. There were no serious complications, such as pulmonary edema or respiratory depression, among the patients included in the study. The patients were classified into those who experienced adverse side effects and those who did not experience adverse side effects. Side effects were febrile sense (n=12), headache (n=6), nausea (n=5), dry mouth (n=5), and loss of the patella reflex (n=1). The I-Mg level tended to be higher in the group with side effects than without side effects. However, it was not statistically significant. Furthermore, the levels of T-Mg, and T-Ca and I-Ca did not show any significant differences.

Comparison of T-Mg and I-Mg levels and T-Ca and I-Ca levels in accordance with presence or absence of adverse effects in patients with preterm labor administered magnesium sulfate
In total, the 64 patients were monitored 165 times. As a result, there was a statistically significant positive correlation between the levels of T-Mg and I-Mg in patients with preterm labor during MgSO4 administration (Fig. 2). Regression analysis obtained the following equation:
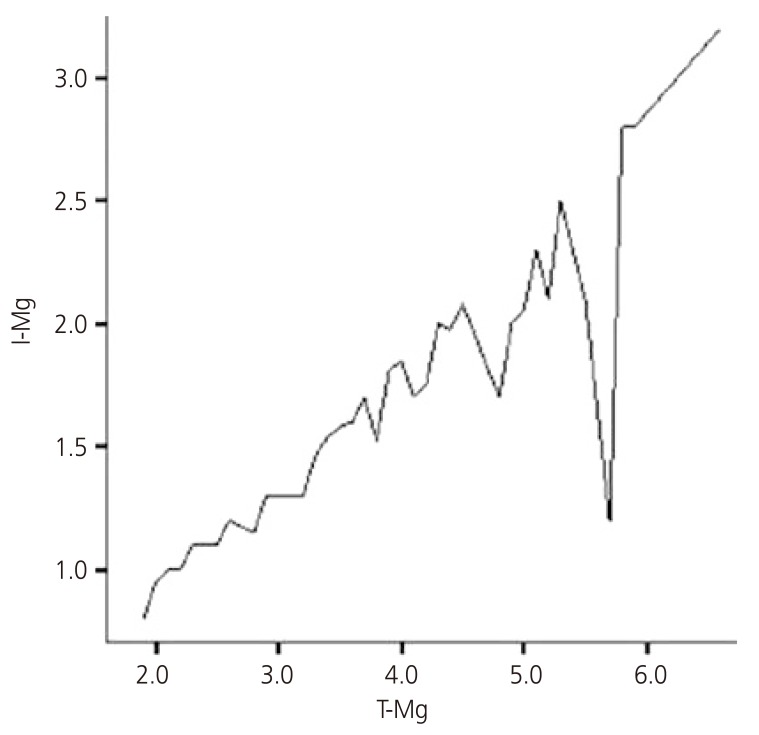
Correlation between ionized and total magnesium (T-Mg) during administration of MgSO4 in patients with preterm labor (n=64). Regression analysis obtained the following equation: Ionized magnesium (I-Mg)=0.395×T-Mg+0.144; F=302.621; P<0.01.
Discussion
According to previous studies, T-Mg has been determined in patients with preterm labor to monitor MgSO4 administration [12]. This measurement includes all 3 fractions of Mg, i.e., the protein-bound fraction, and 2 ultrafiltratable fractions consisting of complex-bound and free I-Mg. However, only the free ionized fraction is biologically active [121718]. Saha et al. [19] compared the use of I-Mg vs. T-Mg in a group of patients with chronic renal disease and found 14 of 69 cases with low T-Mg but normal I-Mg were false-positive for hypomagnesaemia. The authors concluded that T-Mg might overestimate the incidence of hypomagnesemia, and the I-Mg measurement may be beneficial when studying patients with expected hypomagnesemia. Although the study was not targeted at patient with preterm labor, the results support the theory that I-Mg is biologically active. In our data, there was no statistical significance between T- and I-Mg, according to the presence or absence of adverse side effects. However, measurement of I-Mg levels is essential to examine the association between adverse side effects and MgSO4 injection in patients with preterm labor.
In our study, the concentrations of T-Mg and I-Mg were not different between the groups according to the duration of MgSO4 use. Taber et al. [20] studied the pharmacokinetics of I-Mg vs. T-Mg in patients with preterm labor and preeclampsia. In their study, both I-Mg and T-Mg concentrations increased rapidly after standard boluses of MgSO4, with steady-state levels reached within 30 minutes. Interstitial and systemic concentrations of free (i.e., unbound) Mg must be delicately maintained by the combined processes of buffering (binding of ions to proteins and other molecules) and muffling (the transport of ions to storage or extracellular spaces) [21]. It can be inferred that T-Ca and I-Ca maintain equilibrium in a similar way. This supports our argument for the stability of long-term use of MgSO4.
Regarding the association between I-Mg and T-Mg levels during MgSO4 administration, some authors [2223] reported a correlation, while others [20] negated such an association. Taber et al. [20] found a lack of correlation between T-Mg and I-Mg levels in both physiologic and hypermagnesmic (pharmacologic) ranges during MgSO4 administration. The authors suggested that this may be due to variance in total protein concentration or to protein binding or may indicate the presence of buffering systems that control I-Mg within a narrower range than T-Mg. Conversely, Handwerker et al. [22] reported a high correlation between I-Mg and T-Mg for preeclampsia. Also, Yoshida et al. [23] demonstrated a significant correlation between the I-Mg and T-Mg levels during MgSO4 administration for both preterm labor and preeclampsia, supporting the results of our study. These authors speculated that the correlation existed because the mechanism of homeostasis for I-Mg and other forms of Mg might be similar. Therefore, when I-Mg measurement is not possible, our study indicates that it is possible to convert T-Mg to I-Mg level.
In our study, there was no significant difference in I-Ca level before and after administration of MgSO4 in patients with preterm labor. Salamon et al. [24] estimated the effect of MgSO4 concentration on serum I-Mg and I-Ca. They demonstrated that the addition of MgSO4 in vitro causes an exponential increase in serum I-Mg and no significant change in serum I-Ca. Although the in vitro results cannot be entirely extrapolated to the clinical settings, we could have expected a displacement of Ca from its protein- and salt-bound forms, as Mg and Ca are known to compete for these molecules [1]. It is conceivable that MgSO4 administration rarely causes hypocalcemia. However, administration of MgSO4 effects serum Ca through a different pathway — suppressing parathyroid hormone secretion by acting directly on the parathyroid gland, competing with Ca for reabsorption in the loop of Henle and lessening the peripheral actions of parathyroid hormone — that leads to hypocalcemia [25]. Several cases of hypocalcemia [2627] occurring after the MgSO4 administration have been reported. Hence, the T-Ca and I-Ca levels of women receiving MgSO4 therapy should be routinely monitored for hypocalcemia.
This study has limitations. First, our result provides insufficient evidence for the safety of MgSO4 administration. No significant side effects during administration of MgSO4 were observed in our study. This result is probably because the number of participants (n=64) was small and long-term follow-up was not done. Many studies avoid long-term use of MgSO4 in patients because it can induce hypermagnesemia and hypocalcemia [26-29]. Another limitation of our study was the lack of assessment of serum Mg and Ca concentrations and any adverse effects of babies born from mothers treated with MgSO4. Thus, further large-scale research is required to establish the safety of MgSO4 administration. Third, we did not consider any underlying disease in the patients. Indeed, if there are fewer albumin binding sites available for Ca or Mg due to hypoproteinemia, the addition of a small amount of Ca or Mg will have a large effect on the binding of the other ion. Also, serum creatine and body weight significantly affect maternal serum Mg levels.
In conclusion, when MgSO4 was used, Mg and Ca concentrations became equilibrium when certain levels were reached. Furthermore, there was no significant difference between I-Ca levels before and after administration of MgSO4.
Significant correlations exist between I-Mg and T-Mg levels during administration of MgSO4 for preterm labor. Furthermore, the I-Mg level seemed to be more highly correlated with adverse side effects than T-Mg.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.


