



Introduction
Leiomyomas (also known as fibroids, fibromas, fibromyomas, or fibroleiomyomas) are benign tumors composed of smooth muscle cells interlaced in a connective tissue network and bounded by a pseudocapsule of compressed tissue of the adjacent normal myometrium [1]. Multiple tumors in the same uterus are found in up to 84% of affected women [2,3].
Fibroid tumorigenesis is associated with myometrial vascular abnormalities including venular ectasia/increased venous plexus [4-6], arterial dilatation [5], localized expansion of myometrial vasculature [7], and abnormal vascular organization in the perifibroid region [8].
The previously described sonographic vascular features of fibroids include a peripheral rim of vascularity in the pseudocapsule (covering almost three-fourths of their circumference) [9] and marked peripheral flow with decreased central flow/avascular core [10]. This arrangement of leiomyoma vasculature has been termed a “draping” [11] or “spoke-wheel” [12] pattern of vascularization. However, velocimetric indices of fibroid arteries have not been explored in detail.
Doppler sonography of fibroid arteries has been found useful in monitoring leiomyoma response to medical therapy, differentiating leiomyomas from adenomyosis, and assessment of tumor size changes in response to uterine artery embolization (UAE) [13]. Furthermore, the degree of vascularity is said to reflect the likely growth pattern of the tumor and the risk of increased bleeding at surgery [14,15].
The purpose of this study is to evaluate the color Doppler vascularity pattern of uterine fibroid nodules in our environment and the flow velocity indices of their perifibroid and intrafibroid arteries in untreated women and in those with recurrent tumor following previous myomectomy.
Materials and methods
This study was carried out at the Department of Radiology of Obafemi Awolowo University Teaching Hospitals Complex from November 2013 to November 2014. The Institutional Review Board approved the study protocol (approval number: IRB/IEC/0004553).
One hundred and forty premenopausal women with uterine leiomyomas on pelvic sonography were recruited consecutively. Pregnant women, post-menopausal women (cessation of menses >1 year), women with adenomyosis or other pelvic masses, and those with pelvic inflammatory disease were excluded. In addition, all the subjects had normal endometrial plate echo thickness. Women with dominant leiomyoma larger than 4 cm in size after a previous myomectomy were regarded as having recurrent leiomyoma [16]. Subjects' biodata and presence of symptoms (menorrhagia in particular) were ascertained. Informed consent was obtained from all the participants.
A MINDRAY® ultrasound scanner model DC-7 (Shenzhen Mindray Bio-medical Electronics, Nanshan, Shenzhen, China) with a Doppler-enabled convex transducer (frequency of 3.8-5.0 MHz) was used for all the transabdominal sonographic examinations.
The uterus was scanned to determine the number of fibroid nodules, identify the dominant/largest nodule, and assess for presence of degenerative changes. The volume of the dominant nodule was calculated from its length, anteroposterior diameter, and transverse diameter using the ellipsoid formula [17];
The dominant leiomyoma volume was divided into large and small if greater than or less than 200 cm3, respectively [18].
Dominant fibroid nodule vascularity was determined with color Doppler as vascular or avascular. The vascular fibroids were further characterized as having peripheral vascularity only or peripheral and central vascularity. Peripheral vascularity refers to the presence of perifibroid (capsular) arteries only while peripheral+central vascularity denotes the presence of both perifibroid (capsular) arteries and intrafibroid (core) arteries simultaneously/concurrently.
Doppler velocimetric measurements were obtained from the perifibroid (capsular) and/or intrafibroid (core) arteries of the dominant fibroid nodule using a Doppler gate sample volume of 1 mm placed in the centre of the vessel and a Doppler insonation angle of less than 60°.
The following parameters were obtained from an autotrace of the spectral waveform pattern: peak systolic velocity (PSV), end-diastolic velocity (EDV), systolic-diastolic ratio (SDR or S/D ratio=PSV/EDV), resistive index (RI=[PSV−EDV]/PSV), pulsatility index (PI=[PSV−EDV]/[{PSV+EDV}/2]), time-averaged maximum velocity (TAMX), and time-averaged mean velocity (Tmean). The impedance index (ImI=[S× D]/D2) [19] and the diastolic average ratio (DAR=EDV/TAMX) [20] were then derived from the auto-calculated indices. The blood velocity waveforms with the lowest Doppler indices or highest velocities were used for data analysis.
Data was analyzed with the Statistical Package for Social Sciences (SPSS) version 20 for Windows (SPSS Inc., Chicago, IL, USA). The Doppler indices were not normally distributed; therefore, Mann-Whitney U test was used to compare means while the Spearman correlation analysis was used to assess the level of correlation between variables. The χ2 test was used compare 2 categorical variables while Kruskal-Wallis test was used when more than 2 variables were compared. The level of statistical significance was set at P≤0.05. Friedman's analysis of variance and related samples Wilcoxon signed-rank test were also applied as appropriate.
Results
The mean age of the subjects was 37.9±7.4 years. Degenerative changes were observed in 69 (49.3%) subjects: 35 (25%) had cystic degeneration, 22 (15.7%) had calcific degeneration while 12 (8.6%) had both cystic and calcific degenerations.
The median volume of the dominant leiomyoma nodule was 133 cm3 (range=1.5-2,575 cm3). Eighty-three subjects (59.3%) had a dominant leiomyoma nodule volume of ≤200.0 cm3 while the volume of the dominant leiomyoma nodule was >200.0 cm3 in 57 (40.7%) subjects. The dominant fibroid nodule was vascular in 137 (97.9%) subjects and avascular in 3 (2.1%). Seventy-five (53.6%) of the vascular dominant nodules showed peripheral (perifibroid) vascularity only while 62 (44.3%) showed both peripheral and central (intrafibroid/core) vascularity (Figs. 1 and 2).
Fig. 1
Longitudinal triplex sonogram of a myomatous uterus showing the waveform pattern and Doppler indices of a perifibroid (peripheral) artery.
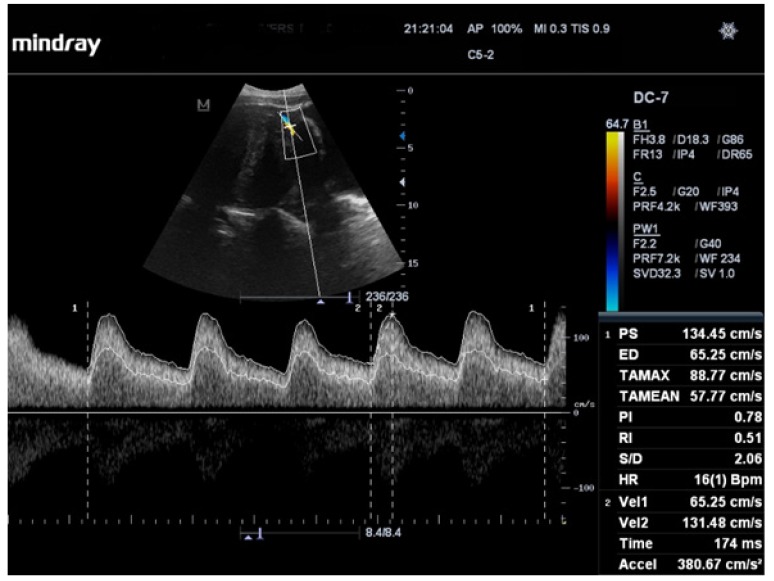
Fig. 2
Longitudinal triplex sonogram of a myomatous uterus showing the waveform pattern and Doppler indices of an intrafibroid (core) artery.

The degree of vascularity increased significantly with increase in dominant fibroid volume. The dominant nodules with both perifibroid and intrafibroid vascularity had significantly larger mean volume (426.26 cm3) than those with perifibroid vascularity only (mean volume=307.27 cm3). These in turn had a mean volume which was significantly larger than that of the avascular dominant nodules (49.27 cm3); P=0.004.
There was no statistically significant difference between the degree of vascularity of myomas with degenerative changes and those without. Similarly, no statistically significant difference was observed between the degree of vascularity of the dominant fibroid nodules in symptomatic subjects and those of asymptomatic subjects. All the perifibroid artery indices (except EDV and DAR) were statistically significantly higher than those of the intrafibroid artery (Table 1). Dominant fibroid nodules with volumes >200 cm3 had statistically significantly higher perifibroid artery DAR and velocimetric indices (PSV, EDV, TAMX, and Tmean), but lower resistance indices (PI, RI, SDR, and ImI) than nodules with volume ≤200 cm3 (Table 2).
Table 1
Comparison of the fibroid artery Doppler indices of subjects
PFA, perifibroid artery; IFA, intrafibroid artery; vs., post hoc analysis; PSV, peak systolic velocity; EDV, end-diastolic velocity; TAMX, time-averaged maximum velocity; Tmean, time-averaged mean velocity; PI, pulsatility index; RI, resistive index; SDR, systolic-diastolic ratio; ImI, impedance index; DAR, diastolic average ratio.
a)Friedman's analysis of variance applied; b)Related samples Wilcoxon signed-rank test applied for post hoc analysis.
Table 2
Effect of dominant fibroid nodule volume on perifibroid artery Doppler indices
PSV, peak systolic velocity; EDV, end-diastolic velocity; TAMX, time-averaged maximum velocity; Tmean, time-averaged mean velocity; PI, pulsatility index; RI, resistive index; SDR, systolic-diastolic ratio; ImI, impedance index; DAR, diastolic average ratio.
a)Mann-Whitney U test applied.
There were no statistically significant differences between the intrafibroid artery velocimetric indices and DAR of dominant nodules with volume ≤200 cm3 and those larger than 200 cm3. However, the intrafibroid PI, RI, SDR, and ImI of the dominant nodules >200 cm3 were significantly lower (Table 3). Subjects with previous myomectomy had significantly higher intrafibroid PI, RI, SDR, and ImI than those without previous myomectomy (Table 4). There were no statistically significant differences between the perifibroid artery Doppler indices of the 2 groups. The perifibroid artery PSV, EDV, TAMX, and Tmean of fibroids with degenerative changes (58.9±29.5 cm/s, 24.3±14.4 cm/s, 36.0±19.2 cm/s, and 16.7±11.5 cm/s, respectively) were statistically significantly higher (P=0.01 for all values) than those of fibroids without degenerative changes (45.6±16.9 cm/s, 18.0±9.5 cm/s, 27.2±11.9 cm/s, and 11.9±6.6 cm/s, respectively). However, there were no statistically significant differences between the intrafibroid Doppler indices of these 2 groups.
Table 3
Effect of dominant fibroid nodule volume on intrafibroid artery Doppler indices
PSV, peak systolic velocity; EDV, end-diastolic velocity; TAMX, time-averaged maximum velocity; Tmean, time-averaged mean velocity; PI, pulsatility index; RI, resistive index; SDR, systolic-diastolic ratio; ImI, impedance index; DAR, diastolic average ratio.
a)Mann-Whitney U test applied.
Table 4
Effect of previous myomectomy on intrafibroid artery Doppler indices
PSV, peak systolic velocity; EDV, end-diastolic velocity; TAMX, time-averaged maximum velocity; Tmean, time-averaged mean velocity; PI, pulsatility index; RI, resistive index; SDR, systolic-diastolic ratio; ImI, impedance index; DAR, diastolic average ratio.
a)Mann-Whitney U test applied.
The EDV, TAMX, and Tmean of the subjects' perifibroid artery correlated positively significantly with the volume of the dominant fibroid nodule (r=0.4-0.5, P<0.001) while the perifibroid artery PI, RI, SDR, and ImI correlated negatively significantly (r=−0.4, P<0.001) with the dominant fibroid nodule volume (Table 5). Only the intrafibroid artery PI, RI, SDR, and ImI significantly correlated inversely (r=−0.5, P<0.001) with the dominant fibroid nodule volume (Table 5).
Table 5
Correlationa) between dominant fibroid nodule volume and Doppler indices of fibroid arteries
PSV, peak systolic velocity; EDV, end-diastolic velocity; TAMX, time-averaged maximum velocity; Tmean, time-averaged mean velocity; PI, pulsatility index; RI, resistive index; SDR, systolic-diastolic ratio; ImI, impedance index; DAR, diastolic average ratio.
a)Spearman correlation applied.
The perifibroid and intrafibroid Doppler indices did not differ significantly between symptomatic and asymptomatic subjects. Similarly, no statistically significant differences were noted between the perifibroid and intrafibroid arteries Doppler indices of subjects with menorrhagia and those without.
Discussion
Fibroid vascularity and flow patterns can be assessed with Doppler sonography [21]. Fibroid nodule vascularity was demonstrated in 97.5% of subjects in this study. This is similar to 100% reported by Sosic et al. [22] and 91% reported by Szabo et al. [23] but much higher than the 70.3%, 51.5%, and 34% reported by Kurjak et al. [24], Tsuda et al. [15], and Samani et al. [25], respectively. The much higher percentage vascularity in this study could be explained by the fact that the fibroid nodules in this study were much larger than the fibroid nodule sizes reported by the authors with lower percentage vascularity. This observation is supported by the fact that the degree of vascularity in this study increased significantly with dominant fibroid volume, such that the dominant nodules with both peripheral and central vascularity had significantly larger mean volume (mean volume=426.3 cm3) than those with peripheral vascularity only (307.3 cm3), whose mean volume was also significantly larger than that of the avascular dominant nodules (49.3 cm3); P=0.004. A similar pattern was documented by Sosic et al. [22] who reported that larger myomas were more vascular than smaller myomas in their study. In fact, they asserted that “of several factors (including menopausal status, phase of menstrual cycle, duration of menopause, size of myomas, location of myomas, and secondary changes within the myomas); the size of the myomas was the most important single factor in determining both visualization of blood flow/vascularity and RI [22]. With an increase in size, a gradual increase in the percentage of visualized flow was noted in all locations, reaching a value of almost 100% in myomas larger than 40 mm [22].” The very low vascularity (34%) reported by Samani et al. [25] might have been due to their small sample size of 15 patients, as well as the smaller sizes of fibroid nodules in their study. Moreover, detection of vascularity requires careful adjustment of the color Doppler scale to optimize detection of slow flow in the fibroid arteries.
Subjects with previous myomectomy had significantly higher intrafibroid PI, RI, SDR, and ImI than those without previous myomectomy. In other words, resistance to flow was higher in the intrafibroid arteries of subjects with previous myomectomy. A possible explanation for this could be that considerable time is needed for the myometrial vasculature to re-expand/enlarge enough to cause a measurable decrease in intrafibroid artery resistance when myomas recur. In addition, a possible contribution to this Doppler picture from healing by fibrosis, if any, is uncertain but plausible. These intrafibroid artery Doppler differences between post-myomectomy subjects and those without previous myomectomy were not observed in the main uterine artery as we reported previously [26] or in the perifibroid artery of this study.
The perifibroid and intrafibroid arteries originate from the fibroid pseudocapsule which is an integral part of all fibroid nodules except the smallest ones [27]. It is composed of collagen fibers and blood vessels (form a vascular ring called “ring of fire” seen on color Doppler sonography) [27]. Assessment of perifibroid and intrafibroid Doppler indices is clinically useful pre- and post-UAE procedures because the overall tumor vascularity is said to be predictive of the therapeutic outcome of UAE [28,29]. Hypervascular fibroids show more reduction in size post-UAE than isovascular and hypovascular fibroids [30] with disappearance of the intrafibroid vessels [29] and a marked reduction in blood flow to the fibroid [10]. On the other hand, fibroids with PSV >64 cm/s are associated with higher rates of UAE failure [28]. In this regard, it is interesting to note that neither the mean perifibroid artery PSV (52.1±24.7 cm/s) nor the mean intrafibroid artery PSV (45.4±28.9 cm/s) obtained in this study is up to this threshold of 64 cm/s.
We did not observe any significant differences between the degree of vascularity of the dominant fibroid nodules in symptomatic subjects and those of asymptomatic subjects. This agrees with the findings of Tsuda et al. [15] of no significant correlation between occurrence of symptoms and presence of leiomyoma/fibroid artery. Furthermore, the perifibroid and intrafibroid Doppler indices did not differ significantly with presence or absence of symptomatology generally and menorrhagia specifically. This is in contrast to previous report [26] of significantly higher PSV, EDV, TAMX in the main uterine artery of symptomatic subjects as well as higher main uterine artery flow velocities and lower resistance to flow in those with menorrhagia. Furthermore, Sladkevicius et al. [31] reported “much higher TAMX values from the arteries supplying the large myomas of the symptomatic premenopausal women than from those supplying the small myomas of the asymptomatic postmenopausal women.” However, we are of the opinion that the documented elevated TAMX by Sladkevicius and co-workers [31] is more likely due to the difference in the myoma sizes of the 2 groups.
Tsiligiannis et al. [32] reported that the mean PSV was significantly higher in the perifibroid region than within the fibroids (30.2 vs. 12.0 cm/s; P<0.001). This is in agreement with our results though we recorded much higher PSV values (54 vs. 45 cm/s; P<0.001), presumably because the leiomyoma nodules in this study are larger. Similarly, the mean perifibroid artery TAMX in this study (31.5±16.4 cm/s) is much higher than that reported by Chiang et al. [33] (10.0±4.5 cm/s).
Fibroids with degenerative changes had significantly higher PSV, TAMX, and Tmean but significantly lower EDV than those without degenerative changes. Szabo et al. [23] reported a similar pattern for PSV in nodules with degenerative changes but our findings differ regarding PI and RI. While they reported a marked reduction of PI and RI in necrotic/degenerative nodules, we found no differences between the PI and RI of those with degenerative changes and those without.
Another vital area where Doppler sonography of fibroid vascularity and velocimetry is of practical clinical use is in the medical management of uterine leiomyomas. Creighton et al. [34] and Yosry et al. [35] demonstrated diminished fibroid volume, reduced fibroid artery velocity, increased fibroid artery PI, and increased fibroid artery RI on therapy with 2 different pharmacologic agents (Gonadotrophin-releasing hormone agonist, Goserelin and aromatase inhibitor, Letrozole). This further emphasizes the clinical importance of Doppler sonographic evaluation of fibroid arteries.
The perifibroid EDV, TAMX, Tmean correlated positively (r=0.4-0.5, P<0.001) while the perifibroid PI, RI, SDR, and ImI correlated negatively (r=−0.4, P<0.001) with the dominant fibroid nodule volume. Furthermore, the intrafibroid artery PI, RI, SDR, and ImI significantly correlated inversely (r=−0.5, P<0.001) with the dominant fibroid nodule volume. Our results are broadly similar to the findings of Huang et al. [36] who assessed the intratumoral/intrafibroid PI of uterine myomas and found a statistically significant inverse correlation between the size of the myoma and PI (r=−0.47, P=0.003), a significant inverse correlation between intrafibroid PI and tumor volumes (r=−0.42, P=0.008), but no correlation between the intrafibroid PI and cell proliferation or angiogenesis. In the same vein, Testa and co-workers [37] reported an inverse correlation between the volume of the myomas and the intratumoral RI (r=−0.46, P=0.012).
The limitations of our study are as follows: Firstly, the sonographic diagnosis of leiomyoma was not confirmed with histology. However, this is mitigated because the accuracy of sonographic diagnosis has improved vastly with advanced technology of modern ultrasound machines. Secondly, leiomyoma and adenomyoma (focal adenomyosis) are difficult to differentiate at sonography (the age of the patient, clinical symptoms, and color Doppler vascularity pattern are vital to differentiating them). The vascular pattern for leiomyoma shows multiple peripherally located vessels surrounding the tumor and, when only a few vessels surround the tumor, these vessels are longer than 1 cm. For focal adenomyosis, the intratumoral signals usually present without peripherally located vessels, and if peripheral vessels are present, they are less than 1 cm long [33]. Thirdly, the more the number of myoma nodules in a uterus, the more difficult it is to identify all the nodules and differentiate one from another. However, we used only the dominant/largest nodule for analysis in this study. Lastly, uterine leiomyoma and uterine sarcoma are virtually impossible to differentiate sonographically. However, sarcoma is very rare with an incidence of 1:500 among patients with presumed leiomyoma [22]. Furthermore, sarcoma is seen almost exclusively in post-menopausal women who were excluded from this study.
We conclude that leiomyoma nodules in our environment are highly vascular. Their predominant pattern of vascularity is peripheral vascularity. Generally, all the perifibroid artery indices (except EDV and DAR) are higher than those of the intrafibroid artery. Recurrent fibroids in women with previous myomectomy show significantly higher intrafibroid PI, RI, SDR, and ImI than those without previous myomectomy.






")











