



Introduction
Epithelial ovarian cancer (EOC) remains the most lethal gynecologic cancer and a leading cause of cancer-related death in women worldwide [1]. Epidemiologic analysis has shown the incidence of EOC increases with age and peaks in the seventh decade of life [2], and that approximately 85% of elderly patients present with stage III or IV disease [3,4]. Patients older than 65 years with advanced stage disease have poor 5-year survival rates which are only one half of those observed for women under 65 years [5]. Elderly patients usually have comorbid diseases, functional disabilities, subsequent increase of the susceptibility to treatment related toxicity, and limitations of standard-of-care treatments. Therefore, effective biomarkers are required that accurately predict prognosis in elderly patients with EOC.
Accumulating evidence indicates inflammation plays critical roles in the initiation and progression of various cancers. Several prognostic indicators from peripheral blood have been widely investigated as potentially useful prognostic markers in different cancers. Of these potentially useful predictors, neutrophil-to-lymphocyte ratio (NLR), the ratio of absolute neutrophil count to absolute lymphocyte count (ALC), has been shown to be associated with poorer pathologic features, such as, an advanced tumor stage, poor progression-free survival (PFS), and poor overall survival (OS) in ovarian cancer [6,7]. Furthermore, elevated preoperative platelet-to-lymphocyte ratio (PLR), that is, the ratio between platelet count and ALC, has been demonstrated to be associated with advanced stage and decreased survival in ovarian carcinoma [8,9]. Preoperative lymphocyte-monocyte ratio (LMR) is another valuable predictor of survival in patients with solid tumors of, for example, the head and neck, breast, lung, and cervix [10,11,12,13].
The prognostic and predictive values of several preoperative hematologic parameters have been investigated in EOC, but evidence regarding the use of LMR as a predictor of outcome in elderly patients with EOC is lacking. Therefore, the aim of the current study was to determine the prognostic significance of preoperative LMR in elderly patients with EOC receiving standard oncology treatment.
Materials and methods
The archived medical records of 42 elderly patients (≥65 years) that underwent primary staging operation and received at least 3 courses of adjuvant platinum-based chemotherapy for EOC between April 2009 and June 2012 were retrospectively investigated. Clinical, pathological, and preoperative complete blood count variables were subjected to analysis. None of the patients received neoadjuvant chemotherapy. Histological diagnoses were based on the World Health Organization criteria, and all microscope slides were reviewed by 2 experienced gynecologic pathologists. Clinicopathologic characteristics including age, performance status, the International Federation of Gynecology and Obstetrics (FIGO) stage, tumor grade, preoperative cancer antigen 125 (CA-125) level, presence of ascites, surgical outcome, and platinum response were collected (Table 1). The study was approved by the Institutional Review Board (IRB) of Pusan National University Hospital (E-2016087).
Table 1
Clinicopathologic characteristics of epithelial ovarian cancer
ECOG, Eastern Cooperative Oncology Group; FIGO, The International Federation of Gynecology and Obstetrics; CA-125, cancer antigen 125.
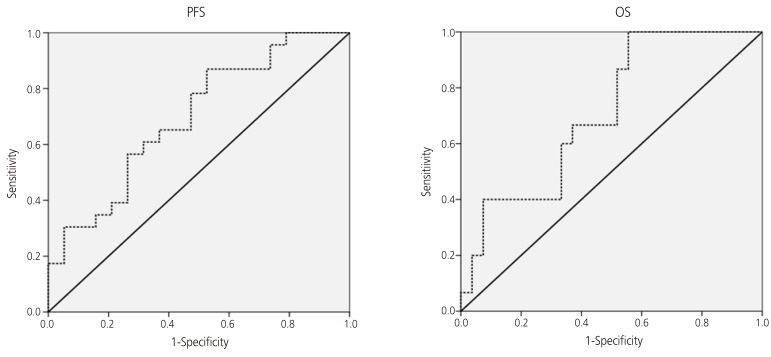
LMR was defined as the ratio of ALC and absolute monocyte count (AMC). Preoperative blood samples were drawn 1 to 2 weeks prior to surgery. Receiver operating characteristic (ROC) curve analysis was used to obtain optimal LMR cut-off values for predicting survival outcomes. The optimal LMR was 3.63, and this value was used as the cut-off for the allocations to LMR-low and LMR-high groups (Fig. 1). The impacts of intergroup LMR differences were evaluated for PFS and OS. The χ2 test was used to analyze differences in proportions, and the differences in survival rates between positive and negative groups were analyzed by means of log-rank test and Cox regression analysis. Data were analyzed using Statistical Package for the Social Science (SPSS) statistical software, version 18.0 (SPSS Inc., Chicago, IL, USA). All presented P-values were 2-sided, and statistical significance was considered at P<0.05.
Fig. 1
Receiver operating characteristic curve analyses showing cut-off points of lymphocyte-monocyte ratio for progression-free survival (PFS) and overall survival (OS) analyses among patients older than 65 years of age with advanced-stage serous epithelial ovarian cancer. The area under the curve for PFS was 0.696 (95% confidence interval [CI], 0.536 to 0.856; P=0.031) and for OS was 0.711 (95% CI, 0.555 to 0.868; P=0.025).
Results
Patient baseline characteristics are presented in Table 1. Median patient age was 70 years (range 65 to 85), and 40.5% were older than 70 years. Serous adenocarcinoma was the most common subtype (78.6%), and 83.3% of patients had a histologic grade of 2 or 3. All patients had an advanced disease stage (III to IV), at initial diagnosis 35 (83.3%) were of stage III and 3 (16.7%) were of IV. Optimal debulking was performed in 30 (71.4%) patients. All 42 patients received at least 3 courses of platinum-based adjuvant chemotherapy after primary surgery, and seven (16.7%) received more than 7 courses. At 6-month postoperative follow-ups after completing platinum-based chemotherapy, 14 (33.3%) patients were classified as platinum resistant and 28 (66.7%) as platinum sensitive.
Regarding the stratification of patients according to the LMR, 29 (69.0%) patients were allocated to the low LMR group and 13 (31.0%) to the high LMR group (Table 2). The 2 groups differed significantly in terms of optimal debulking (P=0.045) and platinum response (P=0.018).
Table 2
Clinical and pathologic characteristics according to the lymphocyte-monocyte ratio (LMR) in epithelial ovarian cancer
Values are presented as number (%).
ECOG, Eastern Cooperative Oncology Group; FIGO, The International Federation of Gynecology and Obstetrics; CA-125, cancer antigen 125.
According to Kaplan-Meier analysis, median PFS and OS for all 42 patients were 42.5 and 68.4 months, respectively. Patients in the high LMR group experienced significant more improvement in PFS (55.2 vs. 33.7 months, P=0.023) and OS (70.0 vs. 59.0 months, P=0.033) than patients in the low LMR group (Fig. 2).
Fig. 2
Progression-free survival (PFS) and overall survival (OS) analysis according to the lymphocyte-monocyte ratio (LMR) in epithelial ovarian cancer.

Age, Eastern Cooperative Oncology Group performance status, clinical stage, histology type, tumor grade, CA-125, optimal debulking, cycles of chemotherapy, platinum response, and LMR were included in both univariate and multivariate analyses. Univariate analysis showed histology type, optimal debulking and platinum response were significantly associated with PFS and OS (all P<0.01), and that LMR was also significantly associated with PFS (P=0.032) and OS (P=0.045). Cox multivariate analysis showed only optimal debulking (PFS, P=0.040; OS, P=0.001) and platinum response (PFS, P=0.001; OS, P=0.003) independently predicted PFS and OS (Tables 3 and 4).
Table 3
Relationship of cancer- and host-related characteristics with progression-free survival in epithelial ovarian cancer
HR, hazard ratio; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; FIGO, The International Federation of Gynecology and Obstetrics; CA-125, cancer antigen 125; LMR, lymphocyte-monocyte ratio.
Table 4
Relationship of cancer- and host-related characteristics with overall survival in epithelial ovarian cancer
HR, hazard ratio; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; FIGO, The International Federation of Gynecology and Obstetrics; CA-125, cancer antigen 125; LMR, lymphocyte-monocyte ratio.
Discussion
EOC is the most lethal gynecologic cancer and a major cause of cancer-related death in women worldwide [1]. This high mortality is mainly due to difficulties associated with early diagnosis and the development of resistance to chemotherapeutic agents and subsequent recurrence. Factors known to influence treatment outcomes in EOC include age, race, FIGO stage, tumor marker, histologic type, tumor grade, and residual tumor after surgery [14]. Age is an important risk factor in the development of ovarian cancer, and for this reason, elderly patients comprise a large proportion of ovarian cancer cases at diagnosis. Several authors have suggested elderly patients have poorer prognoses [15,16], but as yet no definitive evaluation has been conducted on the impacts of biologic and therapeutic features on the relation between survival and age. In order to evaluate the prognostic significance of LMR in elderly ovarian patients, we retrospectively investigated 42 elderly (≥65 years) patients of median age 70 years (range 65 to 85), 17 (40.5%) of whom were older than 70. Although the number of patients included in the present study was relatively small, all patients had advanced stage (III to IV) disease and received at least 3 courses of platinum-based adjuvant chemotherapy after primary staging surgery.
Inflammation is considered a hallmark of cancer, and tumor-associated inflammatory microenvironments are widely regarded to facilitate tumor growth and metastasis. Previous studies have reported hematological markers of systemic inflammation response, such as, NLR, PLR, and LMR, might serve as independent prognostic markers of survival in various cancers. Of these 3 parameters, LMR has been suggested to be associated with survival in malignant lymphoma [17] and in numerous solid tumors [10,11,12,13].
Lymphocytes represent host anti-tumor immune response, inducing cytotoxic cell death, suppressing tumor cell proliferation and migration, and inhibiting cancer dissemination [18]. Monocytes are another type of leucocyte and it has been shown peripheral blood monocyte number is negatively associated with prognosis for different cancer types, which suggests monocytes might independently predict prognoses [19]. Thus, elevated peripheral blood LMR predicts a favorable prognosis in cancer patients. In a previous study, we assessed the prognostic value of LMR in a cohort of 234 EOC patients that underwent surgical resection, and found an elevated LMR was strongly correlated with age, serum CA-125 level, FIGO stage, and the presence of malignant ascites, and that the 5-year PFS and OS rates were better for those with an elevated LMR (PFS, 62.5% vs. 40.0%; P<0.001 and OS, 67.2% vs. 42.2%; P<0.001, respectively) [20]. In a previous multivariate analysis, elevated LMR was found to be strongly correlated with longer survival and to be an independent prognostic factor of survival in EOC patients [8]. Moreover, the present study shows elderly patients in the high LMR group had significantly better PFS (55.2 vs. 33.7 months, P=0.023) and OS (70.0 vs. 59.0 months, P=0.033) than patients in the low LMR group (Fig. 2).
Recent studies demonstrated elderly patients that receive optimal oncologic management have better PFS and OS than those receiving sub-optimal management (median PFS, 18 vs. 11 months; P=0.05 and median OS, 31 vs. 20 months; P<0.001, respectively) [21,22]. The fear of increasing complication rates and the absence of validated selection criteria for treatment decision making in elderly patients are major concerns. In the present study, a high LMR was found to be significantly associated with optimal cytoreduction (92.3% vs. 62.1%, P=0.045) and platinum response (92.3% vs. 55.2%, P=0.018). Furthermore, we found preoperative LMR might predict treatment outcomes in elderly patients with advanced EOC undergoing cytoreductive surgery and adjuvant platinum-based chemotherapy. This study had some limitations that should be addressed, including its retrospective nature and the relatively small number of patients. Further large-scale studies are needed to clarify the prognostic value of preoperative LMR in elderly patients with advanced EOC.
In conclusion, this study is first study to assess the prognostic value of LMR in elderly patients with advanced EOC receiving standard oncology treatment based on LMR. Our results suggest the high LMR is predictive of optimal cytoreduction and sensitive platinum response and longer PFS and OS.






")











