


Introduction
Peritoneal carcinoma is a rare disease with nonspecific symptoms which were pelvic pain, abdominal pain, constipation, bloating, indigestion and abdominal distention. Many imaging studies and biochemical examinations can give a clue to its diagnosis. However, without pathologic confirmation it is able to mimic other peritoneal infectious diseases. We report a rare case which vague symptoms as like constipation, abdominal pain. Tuberculin skin test and abdominal computed tomography (CT) findings presented as peritoneal tuberculosis (TB), but a peritoneal carcinoma was pathologically confirmed. Patients with peritoneal TB mimicking peritoneal carcinoma are common, but the reverse case is rare. Herein, we present, to our knowledge, the first case of a peritoneal carcinomatosis mimicking a peritoneal TB.
Case report
A 57 year old female presented with complaints of abdominal pain for 3 weeks. The pain was dull, aching, and intermittent. She reported a history of constipation, chronic hypertension diagnosed 4 years ago and no history of TB. A history of night sweat, fatigue, weight-loss, and chronic cough or any contact with a pulmonary TB patient was denied. The patient had a previous history of hemorrhoid surgery only.
On clinical examination was the blood pressure 110/70 mmHg, heart rate 76/min and the body temperature 36.8Ōäā. The abdomen was soft, no distended, non-tender and no mass was palpable; but there was a presence of small amounts of ascites. There was no palpable cervical lymph node. Other systemic examinations including cardiovascular system and lungs showed normal results.
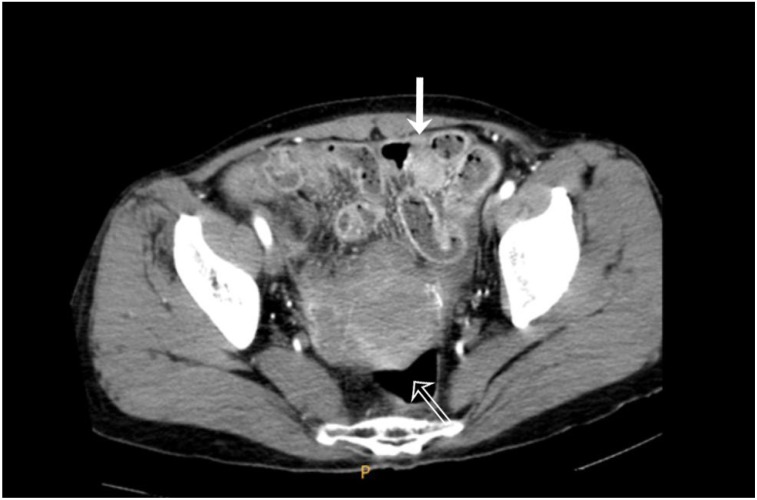
Biochemically, her hemoglobin was 13.3 g/dL, total white cells were 11,940 103/┬ĄL and the C reactive protein was 4.05 mg/dL, otherwise all values were normal. Serum CA-125 levels were elevated (228.6 IU/mL) and serum CA-19-9 levels were normal (<2.0 IU/mL). The chest X-ray was normal. An abdomen CT revealed the presence of an enhancing thickening of the peritoneum, hepatic capsule, omentum and ascites and calcific lymph nodes of the lower abdominal and pelvic cavity (Fig. 1). CT findings suggested a tuberculous peritonitis, but could not rule out a tuberous peritonitis or Fitz-Hugh-Curtis syndrome. The tuberculin skin test result (Mantoux skin test) was positive and interferon-╬│ release assays (QuantiFERON TB Gold, Cellestis, Victoria, Australia) were positive as well. So, a tuberculous peritonitis was suggested for this patient.
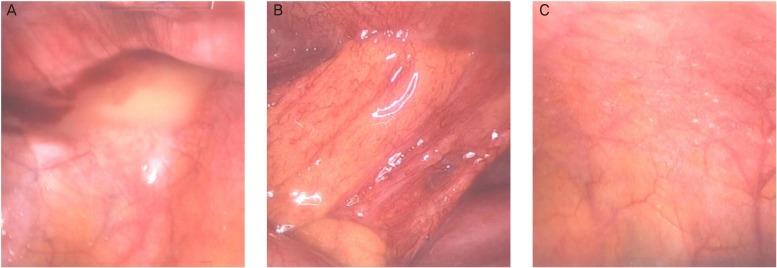
Under this impression, we performed an exploratory laparoscopy for an accurate diagnosis before the TB treatment. There was no mass was observed, neither in the uterus, both ovaries, both salpinges, omentum nor in the peritoneal surface which could be considered as an intraperitoneal malignancy (Fig. 2A, B). Intraperitoneal severe adhesions and small amounts of ascites raised the suspicion of an intra-abdominal tuboovarian abscess. Also suspicious lesion of TB peritonitis was seen (Fig. 2C). Peritoneal washing and peritoneal adhesiolysis was done and a peritoneal ascites probe was sent for bacteriologic and TB evaluation. Also tissue biopsies of the adhesion sites were sent. The acid fast bacilli stain smear test in the peritoneal fluid was negative and the results of Gram stain & bacterial culture were negative as well. The adenosine deaminase in the peritoneal fluid was with 14.0 U/L (6.8-18.2 U/L). No histopathologic evidence of tuberculous granuloma was observed on microscopic examination in the peritoneal fluid. The culture and the examination for a polymerase chain reaction of the sputum did not reveal TB. There was no evidence of TB detected in the lung or pelvic cavity and the patient was subsequently not diagnosed with TB peritonitis but with latent TB therefore.
The pelvic cavity biopsy confirmed the diagnosis of a serous papillary adenocarcinoma. A positron emission tomography (PET)-CT at another hospital revealed a malignancy of both ovary with lymph node metastasis and peritoneal carcinomatosis. After the diagnosis as ovarian cancer, paclitaxel and carboplatin were administered every 3 weeks for treatment.
Discussion
Symptoms of a peritoneal progression from ovarian cancer are nonspecific. Symptoms present are pelvic or abdominal pain, bloating, indigestion and abdominal distention [1]. The patient presented with complaints of abdominal pain but it was not enough to diagnosis.
CA-125 is often used to screen for ovarian, primary peritoneal and fallopian tube cancers in high-risk women. While CA-125 (and other markers) is elevated in most patients with advanced disease, it is not specific for the peritoneal carcinomatosis from an epithelial ovarian cancer. CA-125 may be elevated in many other conditions [1,2]. Serum CA-125 of the patient was elevated, but genital TB may be associated with raised CA-125 also [2].
The role of CT is controversial in the preoperative evaluation of patients with ovarian cancer. Also the role of CT imaging has received little attention and has not been clarified in the recurrent or peritoneal dissemination from ovarian cancer yet. The CT scan plays an important role in the detection of peritoneal carcinomatosis and its mimics. However, the exact diagnosis and characterization of lesions may be difficult due to the overlap of imaging findings [1,3]. Abdominal CT findings of the patient suggested peritoneal TB or pelvic inflammatory disease. Since a precise diagnosis based on imaging findings alone often is not possible, histopathology is mandatory to confirm the diagnosis.
An increased accuracy of PET-CT on peritoneal metastases from an ovarian cancer or the recurrence of ovarian cancer is apparent [1]. Gross operation findings of the patient were unremarkable but PET-CT at another hospital revealed ovarian cancer with peritoneal metastasis. Peritoneal carcinomatosis is a metastatic manifestation of many organ-based malignancies, particularly of carcinomas of the gastrointestinal tract and ovaries and must be considered as the first possibility even in the absence of a known primary. There are several neoplastic and non-neoplastic conditions that may mimic peritoneal carcinomatosis on a CT scan. Those include lymphomas, gastrointestinal stromal tumors, granulomatous infections like TB, and primary peritoneal malignancies such as mesotheliomas [3].
A tuberculous infection of the peritoneum is rarely occurs in developed countries but it is not infrequent in countries with a high prevalence of TB just like Korea [4] and accounts for about 1% to 2% of all cases of TB [5].
It can be difficult and elusive to particularly diagnose a peritoneal TB that may mimic metastases from an ovarian cancer and other nontuberculous granulomatous diseases because of the vague symptoms and nonspecific radiographic, pathologic, and laboratory findings [3].
A peritoneal TB is a form of abdominal TB that involves the omentum, intestinal tract, liver, spleen or the female genital tract in addition to the parietal and visceral peritoneum [5]. Tuberculous peritonitis is seen in combination with a TB of the female genital tract in approximately 45% of patients and is responsible for extensive adhesions, tender abdominal masses, ascites, fever, abdominal pain, weight loss and anorexia [6]. There are great difficulties in its diagnosis due to the non-specific course of the disease. Various methods of investigation have been reported as gold standards; however, there are great difficulties in clinical practice. Routine laboratory and radiographic studies are rarely diagnostic. As a result, the diagnosis of peritoneal TB is still a challenge to the clinician [5].
A strongly positive tuberculin test is sometimes indicative for a reactivation of TB, but the clinical judgement cannot be made solely on this ground since it does not always point to infection and some degree of positivity is seen in patients with prior vaccination also. Therefore, no skin testing for TB was included in the diagnostic work-up of our patients, because the vaccination against this disease is mandatory during early infancy in Korea [7].
Tuberculin skin tests are usually positive in patients with tuberculous peritonitis; however, a negative result doesn't help to exclude the disease [5]. The Mantoux test has a high sensitivity, but, in Korea, the false positive rate counts for 20% if the BCG vaccination was done 12 month after birth. The patient was diagnosed with latent TB before operation. In Korea, the treatment of latent TB depends on the patients' immunity and its medical history [8].
Radiographs of the abdomen are seldom of benefit; however, a CT-scan may be useful in identifying a thickened bowel and ascites [5]. CT features of peritoneal TB include peritoneal thickening, ascites with fine septations, and omental cake [4].
The serum CA-125 levels of this patient were elevated, but no image study suspected a peritoneal carcinoma before surgery in this case. A biopsy is helpful in the differential diagnosis if a peritoneal TB is suspected. The diagnosis of peritoneal TB is often suggested by findings at laparoscopy or laparotomy. Cases of TB mimicking peritoneal carcinoma are common, but a reverse case has not been reported yet. To our knowledge, this is the first case of a peritoneal carcinomatosis mimicking a peritoneal TB.






")











