Increased bone mineral density according to increase of skeletal muscle mass in 534 Korean women: A retrospective cohort study conducted over 2.7 years
Article information
Abstract
Objective
To determine the impact of the changes in the amount of abdominal fat, directly measured by computed tomography, body composition, and the metabolic syndrome (MetS) risk factors on the bone mineral density (BMD) of Korean women.
Methods
A retrospective cohort study involving 534 Korean women aged 29 to 78 years, who had undergone both dual-energy X-ray absorptiometry and abdominal adipose tissue analysis by computed tomography scan more than twice between January 2004 and December 2010. The changes in the BMD values were examined in association with the changes in fat amount, body composition parameters, and risk factors of MetS.
Results
On cross sectional analysis, there was a significant positive correlation between femoral BMD and total abdominal fat amount at the initial visit. However, the correlation disappeared when the impact of change of the fat amount on the change in BMD was analyzed over the study period. When the MetS and body composition parameters were analyzed, a significantly positive correlation was found between skeletal muscle mass and BMD. There was no significant relationship between the MetS risk factors or other body composition parameters and BMD throughout the study period after adjusting for age (time interval).
Conclusion
Among body composition parameters, only increased skeletal muscle mass had a positive correlation with increased BMD over the study period of 2.7 years.
Introduction
Metabolic syndrome (MetS) is defined as a cluster of risk factors for cardiovascular disease (CVD) and diabetes including abdominal obesity, dyslipidemia, hypertension, and glucose intolerance [1,2,3]. Studies that investigated the association between MetS and bone mineral density (BMD) have shown conflicting results varying according to the study population characteristics, such as gender, with some showing positive [4,5], neutral [6,7,8], or negative correlations [9,10,11,12,13,14] thus far. The underlying mechanism leading to the negative correlations is not clear until now; however, low-grade systemic inflammation, which may lead to increased activity of osteoclasts, has been suspected to be the cause, as seen in some cases of autoimmune diseases [15,16].
While abdominal obesity is a major element of MetS, increased body fat has been reported to have a protective effect on the BMD [17]. Although the main impact is thought to be caused by the straining force exerted by the biomechanical load on the bone, the positive correlations between the fat mass and bone density in the non-weight bearing parts of the skeleton were reported to be comparable with those found in weight-bearing parts [18]. Recently, studies have shown differential degrees of association between body fat and BMD when the body fat was divided into subcutaneous and visceral fat components; visceral fat, which is considered to be the major culprit behind the MetS, has been suggested to have an inverse relationship with BMD [19,20,21], while subcutaneous fat, a positive relationship [22], although some studies have shown neutral or inconsistent results on account of their study populations and measurement protocols [23,24,25]. Therefore, we intended to investigate the effect of 'biomechanical load on the BMD' differentially by body fat amount and by skeletal muscle mass (SMM) and that of 'abdominal obesity on the BMD' by compartmental visceral and subcutaneous fat amount.
In addition, to the best of our knowledge, no study has focused on the impact of change in the MetS status or body composition including departmental fat amount and SMM on the change in BMD over a period of several years. Therefore, the objective of this study was to determine the impact of the change in abdominal fat amount, directly measured by computed tomography (CT), body composition, and MetS risk factors on the change in BMD in Korean women over a period of several years.
Materials and methods
1. Study population
This was a retrospective cohort study involving 534 Korean women aged 29 to 78 years, who visited the Seoul National University Hospital Gangnam Center for a routine health check-up program which includes comprehensive physical examinations and various kinds of laboratory and clinical tests and had undergone both dual-energy X-ray absorptiometry and abdominal adipose tissue analysis by CT more than twice between January 2004 and December 2010. In most cases, the examinations and tests are performed on the same date.
The women who had undergone surgical induction of menopause and those who experienced menopause before the age of 45 years were excluded. All patients with chronic debilitating diseases such as malignancies, thyroid disorders, or renal diseases were also excluded. Patient characteristics such as the use of medication (e.g., hormone therapy, antidiabetic drugs, antihypertensive drugs, and lipid-lowering agents), smoking history, reproductive characteristics such as age at menarche, age at menopause, and parity were recorded during a medical interview using a structured questionnaire conducted before a routine gynecologic examination.
Most of the participants voluntarily paid for their health check-ups, while the check-up costs of some patients were borne by their or their spouses' company. This study was approved by the institutional review board of Seoul National University Hospital.
2. Methods
1) Blood sampling and measurement of the anthropometric parameters
Blood samples were obtained from all the participants after a 13- to 15-hour fast. Body weight and height were measured and rounded off to the nearest 0.1 kg and 0.1 cm, respectively. Skeletal muscle mass (SMM), expressed in kg, was measured using a bioelectric impedance analyzer (Inbody4.0, Biospace Co., Seoul, Korea). Waist circumference (WC) was measured at site recommended by the World Health Organization [26] (the midpoint between the lower border of the rib cage and the iliac crest).
2) Measurement of bone mineral density and fat amount
The BMD of the L1-L4, femur necks, and total femurs was measured. Changes in total, visceral and subcutaneous fat amount were measured by abdominal CT (Somatom Sensation 16, Siemens Medical Solutions, Forchheim, Germany). A single slice at the umbilicus level was obtained. The adipose tissue area was determined using commercially available CT software (Rapidia 2.8, Infinitt, Seoul, Korea), and visceral and subcutaneous adipose tissue (SAT) boundaries were defined using a manual tracing method with a cursor, by a single analyzer.
3) Measurement of triglyceride, high-density lipoprotein cholesterol and fasting glucose
The serum levels of triglycerides (TGs) were measured by the HMMPS/Glycerol elimination method, the level of high-density lipoprotein (HDL), by selective elimination method, and the level of fasting glucose, by the hexokinase/G-6-PDH method using a TBA 120 FR device (Toshiba, Tokyo, Japan). The measurement of these values is part of the routine health checkup at our center.
4) Definition of metabolic syndrome
We defined MetS in accordance with the International Diabetes Federation and American Heart Association/National Heart Lung Blood Institute criteria [27], which is based on the major criteria from the National Cholesterol Education Program Adult Treatment Panel III according to which a patient is diagnosed with MetS if 3 or more of the following criteria are met: abdominal obesity (WC in the supine position ≥85 cm for Korean women as proposed by the Korean Society for the Study of Obesity) [28], level of TGs ≥150 mg/dL, HDL cholesterol level <50 mg/dL, high-fasting glucose level ≥100 mg/dL, and blood pressure ≥130/85 mmHg, determined after performing 2 measurements separated by a 10-minutes resting period or if already receiving treatment for these conditions.
5) Statistical analysis
The cross-sectional association analyses among study parameters were analyzed only at visit 1. In addition, longitudinal analyses were performed over the study period, since the health check-up and medical counseling itself at visit 1 might have some degree of effect on the participants' lifestyle toward more health-promoting pattern though there's no tool to evaluate the size of the effect in this study. The continuous variables measured in this study were expressed using mean and standard deviation values. For the statistical analysis, stepwise multiple regression analyses were conducted using the SAS ver. 9.2 (SAS Institute, Cary, NC, USA). Univariate and multivariate logistic regression models were used to identify independent associations between abdominal fat amount (total, subcutaneous, and visceral) and MetS risk factors and BMD at the lumbar and femur at the initial visit and over the study period.
Results
1. Characteristics of the study population
The mean age of the participants was 52.7±8.1 years and the mean follow-up interval was 2.7 years. During the course of the study, 142 (26.6%) women were premenopausal, 304 (56.9%) were postmenopausal, and the remaining 88 (16.5%) were in the menopausal transition period.
Eighty five (15.9%) women had MetS at visit 1, and the number increased to 88 (16.5%) at visit 2. The average numbers of MetS risk factors observed were 1.25±1.24 and 1.22±1.23 at visit 1 and 2, respectively (Table 1).
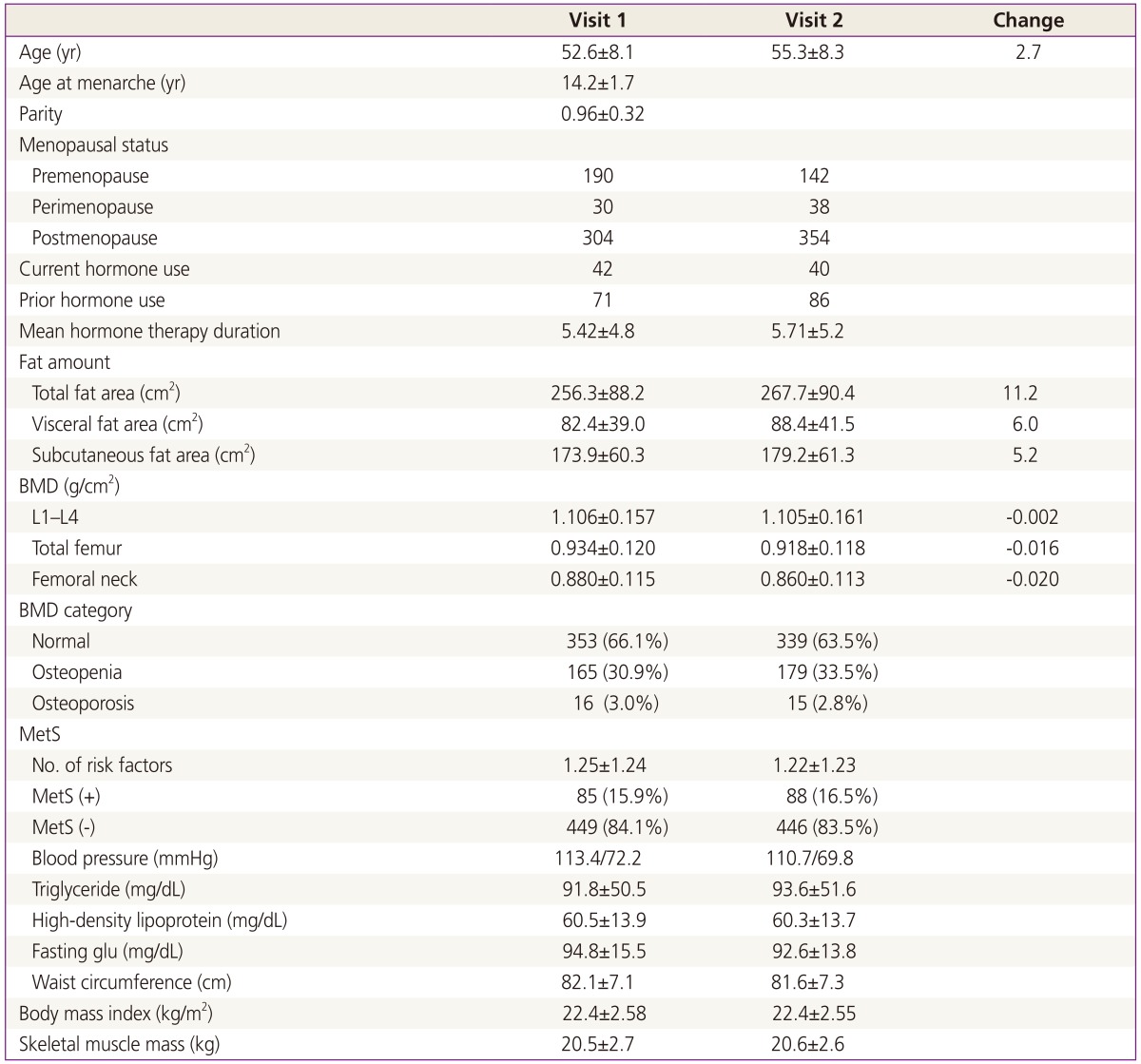
Characteristics of study population, BMD, anthropometric parameters, and MetS markers at Visit 1 and Visit 2
2. Association between bone mineral density and abdominal fat amount, and metabolic syndrome risk factors at visit 1
There was a significantly positive correlation between the BMD of the total femur with total abdominal fat amount, and the significance between BMD and total adipose tissue amount was retained after adjustment for age and menopausal status. On the other hand, there was no significant association between lumbar or femoral neck BMD and abdominal fat amount (Table 2).
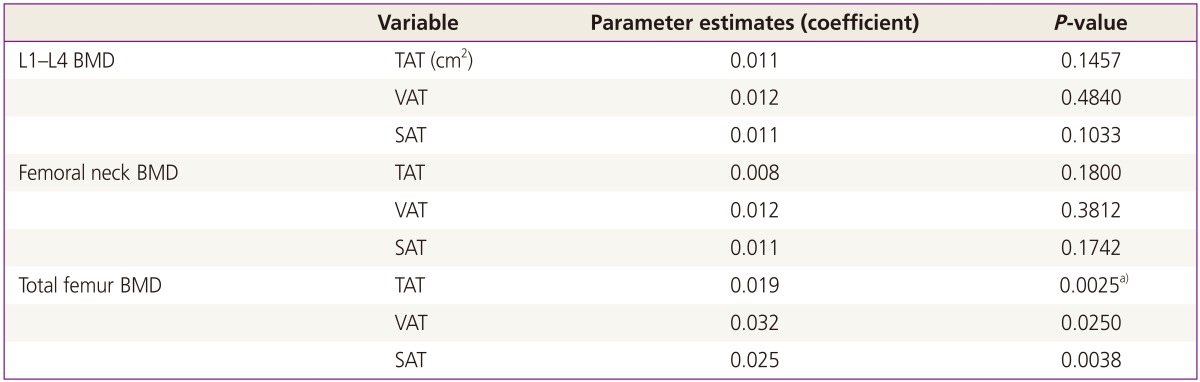
Associations between BMD and fat amount at visit 1
The lumbar and femoral BMD values showed negative and positive correlations with WC and SMM, respectively. In addition, total femoral BMD showed a positive correlation with body mass index, and the significance persisted after adjusting for age and menopausal status (Table 3).

Association between BMD and metabolic syndrome risk factors, age, and menopausal status at visit 1
3. Association between change in bone mineral density and change in fat amount and metabolic syndrome risk factors over the study period
All the correlations between femoral BMD and fat amount disappeared when the impact of change in the fat amount on the change in BMD over time was analyzed. When MetS (WC, TG, HDL, fasting glucose, blood pressure) and body composition parameters were included in the analysis, a significantly positive correlation was found between SMM and lumbar and femoral BMD. Otherwise, there was no significant relationship between any of the MetS risk factors or body composition parameters and BMD throughout the study period after adjustment for age (time interval) (Table 4).
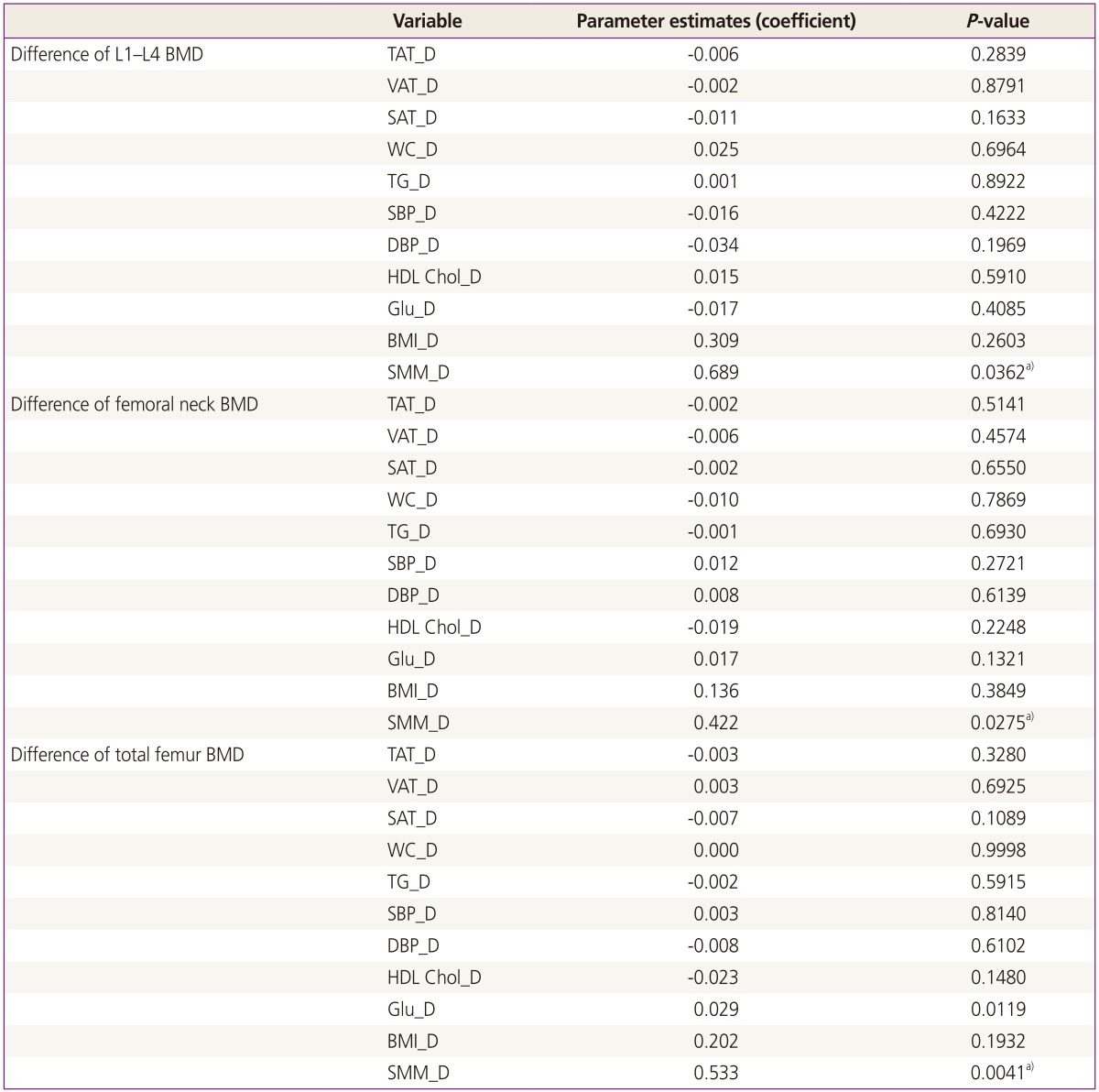
Association between BMD and change in adipose tissue amount and metabolic syndrome risk factors after adjusting for menopausal status, age, and interval between two visits
Discussion
Many studies have focused on the relationship between MetS and BMD. Some of these studies show a protective action of MetS on BMD [4,5,8]. The researchers ascribe this positive correlation to the increased body weight represented by increased WC and stated that despite the increased BMD, there was no reduction in fracture prevalence in the study groups [4]. On the other hand, most of the studies found a negative correlation between MetS and BMD; they suggested that the increased osteoclast activity in chronic systemic low-grade inflammation associated with MetS is the reason behind the negative association [9,10,11,13,14,29]. Most of those studies had a cross-sectional design, and it is usually hard to explain the causal relationship even in cases of significant positive or negative correlations since each of the MetS risk factors are also CVD risk factors. In addition, many studies found no significant correlation between MetS and BMD. Probably, with increasing prevalence of MetS and decreasing mean value of BMD, a significant relation was observed between the two at a specific time point in some study populations.
The protective effect of high body mass index on BMD is well known [30,31,32]. However, studies have shown conflicting results regarding the correlation between body fat and BMD [19,20,21,23,24,25]. Recent studies have also shown that there are biologic and metabolic differences between the SAT and visceral adipose tissue (VAT) present in the abdominal cavity; VAT adipocytes are more metabolically active, sensitive to lipolysis, and resistant to insulin than SAT adipocytes [33]. Studies that focused on the relationship between regional adipose tissue and BMD reported that SAT was associated with increased midtibial periosteal cortical thickness, and VAT, with decreased spinal BMD [20,22]; it should be noted that the study populations in these studies consisted of children and adolescents.
In this study, we intended to examine not only cross-sectional but also longitudinal markers that are significant determinants of BMD changes caused by adipose tissue amount (total, subcutaneous, and visceral) and risk factors of MetS over time in Korean women.
In the cross-sectional analysis, the total amount of adipose tissue was found to be positively correlated with total femoral BMD, but not with lumbar or femoral neck BMD. In the longitudinal analysis, however, we could not find any correlation between the changes in the amount of fat and BMD at any region even after the fat amount was divided regionally and proportionally (SAT/VAT, data not shown). In cross-sectional analysis involving MetS and body composition parameters and BMD values, WC was negatively correlated with the BMD values of the said parts, implying that visceral obesity, expressed as increased WC, is negatively associated with BMD. SMM showed a positive correlation with the BMD values of the said parts. On longitudinal analysis, BMD showed a significant correlation with SMM but not with WC, indicating that retention or increment of muscle mass over time is the most important and significant protective factor in prevention of bone loss in this study population. On longitudinal analysis, however, we could not find any correlation between the change in the amount of fat and BMD values of the all study parts, even after the fat amount was divided regionally and proportionally.
To the best of our knowledge, this is the first study on the relation between the changes in BMD, fat amount, MetS risk factors, and body compositions markers over time, though the study period was a short duration of about 3 years. Although the representativeness of this population of Korean women is questionable, as the study population that visited this center tended to be women who had a high socioeconomic status who could pay expensive private health check-up programs which are not covered by national health insurance, higher proportion of single status (mean parity, 0.96), and high level of health consciousness and motivation (decreased MetS risk factors over study period); this study had a retrospective design; and some important information like exercise was missing, this study showed that maintaining SMM over time (most probably by regular exercise) is the most important factor for maintaining optimal BMD in Korean adult women. This study also confirms that the adipose tissue amount and MetS risk factors are not associated with lumbar or femoral BMD over time.
In our study, the SMM had a positive correlation with BMD over time. In other words, maintaining SMM over time is the most important factor for maintaining optimal BMD in Korean adult women. The change in the amount of body fat or MetS risk factors had no association with the change in lumbar or femoral BMD in Korean women over the study period of 2.7 years.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgments
This paper was supported by Seoul National University Hospital General Research Fund in 2010. We are sincerely grateful to all the participating women. We would like to thank EunKyung Min RN who performed the manual measurements of abdominal fat amount in this study and the Medical Research Collaboration Center of Seoul National University Hospital for the assistance granted in the statistical analyses conducted in this study.