




Introduction
Coronavirus disease 2019 (COVID-19) is a respiratory disease that originated in Wuhan, China in 2019 [1]. COVID-19 is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), with common symptoms including fever, fatigue, dry cough, anorexia, myalgia, dyspnea, and sputum production [2,3]. Pneumonia is one of the most common outcomes in pregnant women with COVID-19 and is associated with increased morbidity and mortality [4]. During pregnancy, it can cause severe maternal complications, including respiratory failure, and is associated with an increased risk of low birth weight and preterm birth of newborns born to women with COVID-19 [5]. Pregnancy-induced physiological changes, such as hormonal changes and elevation of the diaphragm from the pregnant uterus, affect pulmonary function, resulting in poor ability to cope with respiratory diseases during pregnancy [5].
Based on the most recent systematic review and meta-analysis on neonatal outcomes, COVID-19 in pregnant women can have adverse effects on newborns, such as preterm birth, shortness of breath, and neonatal death [6].
Several studies have described the prognosis of pregnant women with COVID-19 and their newborns; however, it is unclear whether COVID-19 increases the rate of adverse obstetric outcomes in pregnant women and their newborns, and data since the first case report in 2020 [7] .
Medical organizations, including the Center of Disease Control and the American College of Obstetricians and Gynecologists, recommend COVID-19 vaccination for pregnant women [8,9]. In South Korea, the types of COVID-19 vaccines are RNA vaccines, including Moderna and Pfizer, and viral vector vaccines, including Janssen and AstraZeneca. According to the Korea Disease Control and Prevention Agency, the Pfizer vaccine is recommended for all Koreans from age 5, including pregnant women. The Moderna vaccine is recommended for all Koreans from age 30, the AstraZeneca vaccine from age 50, and the Janssen vaccine from age 18, which is contraindicated in mRNA vaccines. Concerns regarding COVID-19 vaccination are increasing, as limited data are available on its efficacy and safety; these concerns are particularly salient for pregnant women. In this study, we analyzed the vaccination status of pregnant women in South Korea and compared the prognoses of pregnant women after vaccination based on different types of COVID-19 vaccines. This study aimed to provide important information for the clinical management of pregnant women and their newborns.
Materials and methods
1. Participants
The data in this study were calculated based on the cohort data of 12,399,065 women of childbearing age (aged 15-49 years in 2019-2021) estimated by the Korean National Health Insurance Service. These data include information on the disease and prognosis of pregnant women and newborns based on COVID-19 and pregnancy. They also include reports on the vaccination status of women under the Korean National Health Insurance Service care (mostly Koreans), which started in 2021, as well as their obstetric prognosis after vaccination. The details include the following: (1) prognosis of women, diseases corresponding to codes O00-O94 defined by ICD-10, including cesarean section, which belongs to the category ŌĆ£Pregnancy, childbirth, and the puerperium,ŌĆØ and severe disease, which corresponds to the V code of the category ŌĆ£External cause of morbidity.ŌĆØ The prognoses of pregnant women with COVID-19 and those without infection have been previously described; (2) the prognosis of newborns, diseases corresponding to codes P00-P96, which belong to the category ŌĆ£certain conditions originating in the perinatal periodŌĆØ and neonatal intensive care unit (NICU) information. The prognosis of newborns born to pregnant women with COVID-19 and those born to pregnant women without COVID-19 are described; (3) number of vaccinations performed, description based on the type of vaccine, pregnancy, and age. For pregnant women who were vaccinated during pregnancy, the types of vaccine used, the number of gestational weeks at the time of vaccination, and obstetric outcomes based on the type of vaccine were analyzed.
2. Study participants
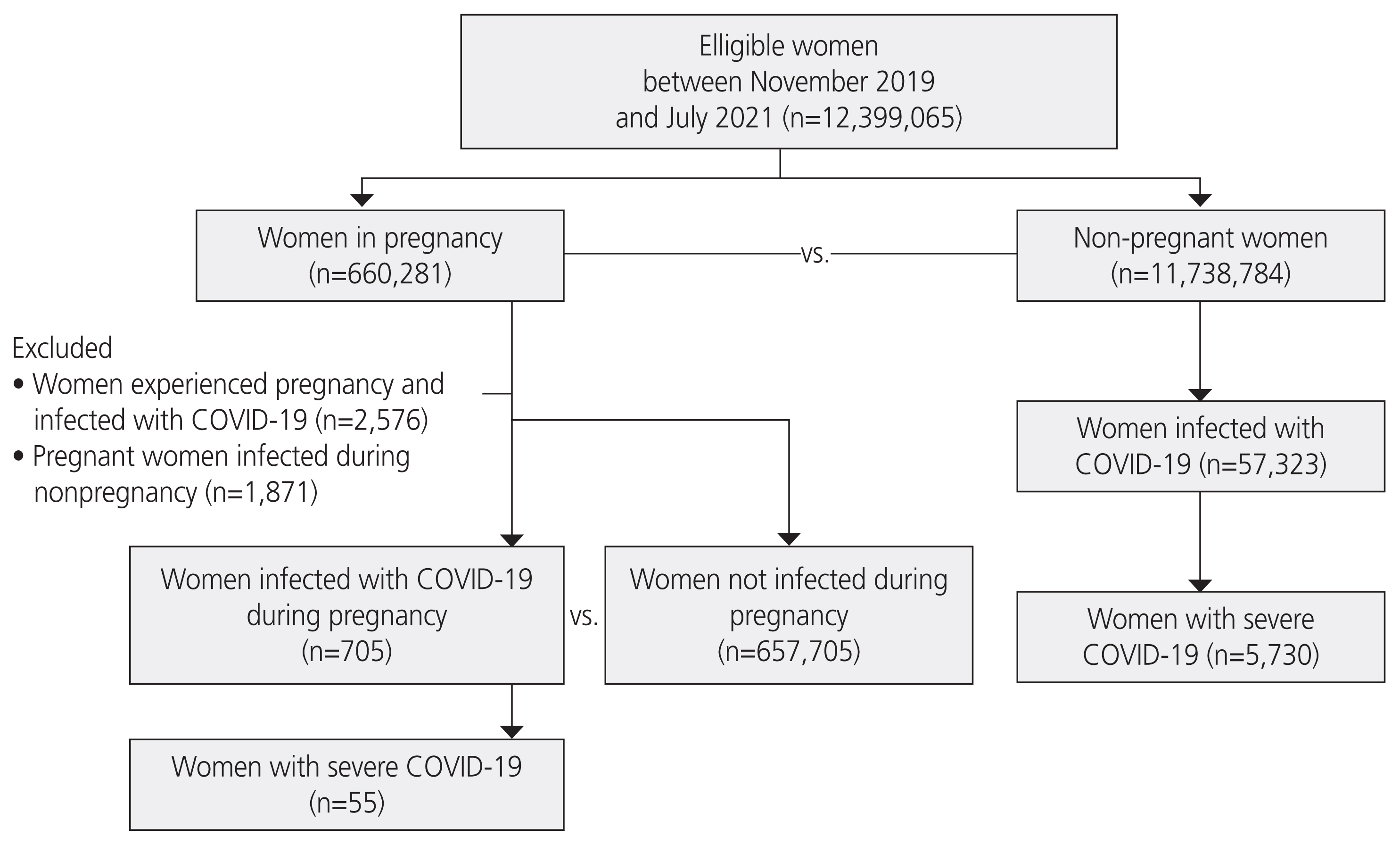
First, non-pregnant (n=1,138,784) and pregnant (n=660,281) women were compared to determine whether COVID-19 has specific effects during pregnancy. Pregnant women were divided into two groups: pregnant women with and without COVID-19. They were compared to determine whether the two groups had different prognoses. In addition, the newborns of these women were compared to determine the effect of COVID-19 on their prognosis. Finally, pregnant women who were vaccinated during pregnancy were analyzed based on vaccine type, number of gestational weeks at the time of vaccination, and obstetric outcomes after vaccination.
3. Statistical analysis
We performed a chi-squared test to compare the distributions of the two groups. However, FisherŌĆÖs exact test was performed for cases in which more than 20% of cells had an expected frequency of <5, since applying the approximation method in these cases was considered inadequate (and the chi-squared test relies on approximation) [10].
Results
Among 12,399,065 women, 59,899 (0.48%) were diagnosed with COVID-19 and 660,281 (5.32%) were pregnant between November 2019 and July 2021 (Fig. 1). Among the women who were pregnant during the study period, 2,576 were diagnosed with COVID-19, corresponding to 0.02% of the total included women and 0.39% of pregnant women. Among them, 705 women were diagnosed with COVID-19 during pregnancy, corresponding to 0.11% of women who were pregnant during the study period. Conversely, 0.89% of the women who experienced pregnancy during the study period were infected in the period before pregnancy. In this study, all women infected during the non-pregnancy period were excluded because we could not confirm the direct relationship between pregnancy and COVID-19. Table 1 shows the percentages of pregnant and non-pregnant women with COVID-19 during the study period. There were 57,323 women (0.49%) with COVID-19 in the non-pregnant group and 705 women (0.11%) in the pregnant group. In a statistical test comparing the rates of COVID-19 in the two groups, the P-value was below 2.2e-16, indicating that the incidence of COVID-19 was lower in pregnant women than in non-pregnant women.
Table 2-1 shows the count, rate, and statistical test results for diseases in pregnant women with and without COVID-19. There was a significant difference between the two groups in the rates of obstetric complications, including diabetes during pregnancy, premature rupture of membranes, suspected cephalopelvic disproportion, postpartum hemorrhage, infection, and venous complications during pregnancy and puerperium (O02, O12, O22, O23, O24, O32, O33, O36, O42, O47, O60, O63, O65, O66, O67, O70, O71, O72, O75, O80, O81, O82, O83, O86, O87, O90, O91, O92, and O94). The rates of these complications were significantly higher in pregnant women without COVID-19 than in those with COVID-19. Table 2-2 shows two prognoses related to childbirth observed in this study among the diseases listed in Table 2-1. Statistical tests showed that the number of preterm births and cesarean sections in pregnant women with COVID-19 was significantly lower than that in pregnant women without COVID-19 (P=0.0024 and <2.2e-16 in preterm birth and cesarean section, respectively).
Table 2-3 shows the proportion of severe diseases based on pregnancy and COVID-19 status. Among the 705 infected pregnant women, 55 (7.8%) experienced severe disease, and among 57,323 infected non-pregnant women, 5,730 (10.0%) experienced severe disease (P=0.0615).
Table 3-1 shows the count, rate, and statistical test results for diseases in newborns born to pregnant women with and without COVID-19. Regarding P00-P96, significantly higher rates of P00 (newborns affected by maternal conditions that may be unrelated to the current pregnancy), P03 (newborns affected by other complications of labor and delivery), and P12 (birth injury to the scalp) were found in the infected pregnant women group (P<0.0001, P<0.0001, and P=0.0412, respectively). In addition, Table 3-2 shows the information on birth weight and NICU admission of newborns based on the maternal status of COVID-19. Newborns born to mothers with COVID-19 were admitted to the NICU at an increased rate of 10.98%. However, there were no significant differences in the proportions of low birth weight and macrosomia between the two groups.
Based on Tables 4-1, 4-2, 264,927 women (2.14%) of the total number of Korean women of childbearing age were vaccinated. In this group, 13,240 women were vaccinated during pregnancy, accounting for 5% of the vaccinations, and 10,429 pregnant women (78.77%) were vaccinated before 28 weeks of pregnancy. The proportion of pregnant women for each vaccine type was 4.26% for Moderna, 5.59% for Janssen, 7.20% for AstraZeneca, and 4.94% for Pfizer. As shown in Table 5, obstetric complications based on ICD-10 codes of women who received the Moderna or Pfizer vaccine were lower than those of women who received the Janssen or AstraZeneca vaccine. In particular, Janssen had a corresponding rate of 3.19% in O00-O08 (pregnancy with abortive outcome), and AstraZeneca had corresponding rates of 4.93% and 3.08% in O00-O08 and O20-O29 (other maternal disorders predominantly related to pregnancy), respectively. Moderna and Pfizer vaccines were associated with <1% of all diseases. In particular, the AstraZeneca vaccine was associated with a higher rate of obstetric complications; however, this may be due to the higher average age of women who received the AstraZeneca vaccine.
Discussion
1. Study findings
Among the pregnant women, 0.11% were diagnosed with COVID-19 during pregnancy. Remarkably, the rate of various obstetric complications, including preterm birth and requirement for cesarean section, was significantly lower in pregnant women with COVID-19 than in those without COVID-19. Only the miscarriage (O02) rate increased in pregnant women with COVID-19 compared to those without COVID-19. Pregnant women with and without COVID-19 presented with approximately the same proportion of severe disease. COVID-19 also had no significant effect on fetal prognosis in almost all cases; however, newborns born to women with COVID-19 were significantly more vulnerable to birth injury to the scalp. In addition, newborns born to women with COVID-19 were more likely to be sent to the NICU. Vaccines were frequently administered within 28 weeks of pregnancy, and AstraZeneca and Janssen vaccines were associated with worse obstetric outcomes than mRNA vaccines, such as Pfizer and Moderna.
2. Study contribution
In this study, COVID-19 did not have a fatal effect on pregnant women and fetuses; however, COVID-19 was associated with an increased rate of miscarriage in early pregnancy. Remarkably, the results showed that pregnancy complications decreased in mothers diagnosed with COVID-19 during pregnancy. The lower complication rates and relatively good obstetric outcomes of COVID-19 during pregnancy indicate that acquiring this infection during pregnancy may not result in adverse outcomes, or that both pregnant women infected with COVID-19 and the medical staff were already aware of the potential implications of this infection. The most common SARS-CoV-2 variants in South Korea during the study period were B.1.1.7 (alpha) and B.1.620, which were different from other variants that were prevalent worldwide at that time (https://covariants.org/per-country). Different distributions of viral variants may be associated with good obstetric outcomes. Pregnant women with COVID-19 had a lower rate of preterm births and cesarean sections than those without COVID-19, and the rate of severe disease did not differ significantly between these groups. These results are not consistent with those of the United States Centers for Disease Control and Prevention COVID-19 surveillance system, in which pregnant women with COVID-19 were more likely to experience preterm birth or other adverse birth outcomes than those without COVID-19 [11,12]. Further studies are needed to clarify these conflicting results.
The phenomenon of lower preterm birth and cesarean section in pregnant women with COVID-19 require careful assessment. Several studies have reported a higher rate of preterm birth and cesarean section in pregnant women with COVID-19; however, some results are contradictory [13-20]. In addition, the most frequent causes of early emergency cesarean sections were reported to be fetal distress and worsening respiratory symptoms in pregnant women with COVID-19 [20]. There are several reasons that may contribute to the fact that pregnant women with COVID-19 had a low rate of preterm birth and cesarean section in our study compared to the results of several other studies.
First, this study used extensive and relatively updated data from November 2019 to July 2021. In a previous study, authors hypothesized that the rate of cesarean section decreased as experience in managing pregnant women with COVID-19 increased, since vaginal delivery does not appear to be associated with worse results in pregnant women or their newborns than cesarean section. Therefore, it seems appropriate that in our study, which included recent data, there was a lower rate of preterm birth and cesarean section associated with COVID-19.
Another reason that our results differ from those of some previous reports is that preterm birth or cesarean section may have been underreported among pregnant women with COVID-19, and it may be because many pregnant women with COVID-19 did not present to medical facilities out of fear. Strong support from medical facilities and staff is vital for pregnant women with COVID-19. Another explanation may be the changes in clinical practice due to the pandemic, which may have lowered the incidence of cesarean section or preterm birth among pregnant women with COVID-19 [21]. Although many complex factors must be considered regarding delivery timing and mode, infected women may have had reduced in-person appointments with obstetricians and, therefore, may not have undergone some interventions, such as labor induction.
Another explanation for the lower preterm birth rate in pregnant women with COVID-19 is modified behavior, such as wearing masks, washing hands, reduced physical exercise, reduced work-related stress, and earlier conservative treatment followed by quarantine, which results in a lower rate of infection from any source that may lead to preterm birth. This phenomenon was demonstrated in China and the UK before and after the pandemic, in which the preterm birth rate was lower after the pandemic [22,23].
Finally, another explanation is that pregnant women and fetuses receive special protection based on KoreaŌĆÖs COVID-19 response guidelines in circumstances where the infection itself does not seriously affect obstetric outcomes. South Korea used the ŌĆ£Three T Strategy,ŌĆØ which stands for testing, tracing, and treatment, enabling early detection and treatment of COVID-19 [24]. This strategy has ultimately led to low morbidity and mortality in the general population and maternity care regarding COVID-19, predominantly delta type, before December 2021, when the omicron type was not prevalent. During this period, pregnant women with COVID-19 or symptoms should notify infection specialists, obstetricians, and pediatricians before and during delivery, followed by quarantine to prevent the spread of infection to other people, and at the same time, doctors should immediately prepare appropriate plans based on the clinical conditions of pregnant women with COVID-19. Recently, in South Korea, the predominant type of COVID-19 has changed to omicron, which is a milder type with lower mortality, but spreads more easily. The fourth outbreak started in December 2021 and peaked in March 2022. The pandemic response strategy 3T against delta type has transformed into a new strategy because this milder omicron type causes more flu-like symptoms with lower fatality. To date, the fatality rate is approximately 0.13-0.15% and even lower in pregnant women. With the surge of COVID-19 in March 2022, the rate of infection has decreased and South Korea is about to reach the endemic stage.
The Korean government adopted a universal health coverage model during the COVID-19 pandemic in which all expenses related to COVID-19 are covered by the government, starting from 1st patient with COVID-19 in January 2020, which guided accessibility to medical care [25]. Due to the facilitated accessibility to health services, when pregnant women are diagnosed with COVID-19, they receive medical care before their symptoms worsen and the disease progresses. Indeed, in our study, there was no significant difference between the two groups regarding the proportion of severe diseases, unlike previous studies that described pregnant women with severe COVID-19 and adverse pregnancy outcomes, including intensive care unit admission [26]. In addition, in Korea, newborns born to pregnant women with COVID-19 or pregnant women presenting with COVID-19-related symptoms are quarantined in a negative-pressure bed in the NICU, regardless of whether intensive care is needed. Therefore, the NICU admission rate of newborns born to women with COVID-19 was significantly higher than that of newborns born to women without COVID-19. Therefore, with appropriate management, COVID-19 appears to have little effect on pregnant women and their fetuses. However, the rates of P3 (fetuses and newborns affected by other complications of labor and delivery) and P12 (birth injury to scalp) were significantly higher in fetuses of pregnant women with COVID-19 than in those of pregnant women without the infection. This prognosis is possibly due to the fact that more time is needed to prepare for delivery in pregnant women with COVID-19, and operative delivery is more likely to be adopted to shorten delivery time to avoid the spread of virus. Further studies are required to improve our understanding of these results. There is much evidence in the literature that vaginal delivery can be a risk factor for birth injury to the scalp, while cesarean delivery can be a protective factor [27,28]. Based on the data, we considered whether high birth injury to the scalp (P12 code) in neonates born to pregnant women with COVID-19 is related to the fact that this group had a low cesarean section rate, that is, a high vaginal delivery rate. The delivery mode appears to have a greater impact on perinatal outcomes than COVID-19 status.
Based on the results of the analysis of adverse reactions after vaccination released by the Korea Central Disease Control Headquarters, the rates of adverse reactions associated with the AstraZeneca and Janssen vaccines were 26.3% and 24.5%, respectively, which were higher than those of the Moderna and Pfizer vaccines (10.6% and 13.7%, respectively). The prognosis of pregnant women who received the AstraZeneca and Janssen vaccines was worse than that of pregnant women who received the Moderna and Pfizer vaccines because of the nature of the former two vaccines, which causes many abnormal symptoms, such as muscle ache, fever, fatigue, headache, Guillain Barre syndrome, and thrombocytopenia. In practice, mRNA vaccines such as Moderna and Pfizer have been reported to be safe for pregnant women and their fetuses [29]. A recent clinical study demonstrated no increased risk of preterm birth and no ŌĆ£small for gestational ageŌĆØ status after COVID-19 vaccination during pregnancy [30]. Therefore, at present, pregnant women are recommended to be vaccinated with mRNA products associated with fewer abnormal symptoms; however, further research is needed to clarify these results.
3. Study limitations
This study had several limitations. (1) All patients diagnosed with COVID-19 during the study period, in which infection did not occur during pregnancy, were excluded. Patients were also excluded if information regarding the timing of COVID-19 onset and pregnancy was unavailable. (2) Since this study was analyzed based on the National Health Insurance Claims database of South Korea, detailed medical information was not available from this database. For instance, if we had been able to examine the diagnostic codes, medications, and treatment data of 26 newborns who were hospitalized in the NICU after being born to mothers with COVID-19, it would have been clear whether these newborns needed intensive care. Due to data limitations, further analysis was difficult. Meanwhile, there was a higher rate of obstetric complications and a lower rate of spontaneous, operative, and other assisted single deliveries in our study population. Nevertheless, because the retrieved data were random, we did not choose certain preferable patients. (3) Owing to the known side effects of vaccines [31] and the countryŌĆÖs vaccination policy, the vaccination age range is not uniform for each vaccine. For example, the Janssen vaccine has only been administered to individuals over 30 years of age. It is already known that childbirth at an older age is highly risky and associated with a poor prognosis compared to childbirth at a younger age, and it includes risks such as preterm birth and Down syndrome. Therefore, age should be considered as an important factor in this study. However, we were provided with limited information regarding age; therefore, were not able to analyze age. (4) In this study, it was necessary to count each ICD-10 code, that is, 206 for O20 and 144 for O21 in the infected pregnant women group. However, several ICD-10 codes often correspond to the same disease. For example, to determine whether hypertension in pregnancy is applicable, we must also consider O10-16. However, we were provided with a count for each ICD-10 code, except for a few cases. Furthermore, because there may be overlapping targets between codes, we cannot arbitrarily combine them. And (5) in South Korea, all four types of vaccines were permitted between February and May 2021, and it has been recommended since October 8, 2021 that pregnant women should undergo vaccination. Considering the study period (November 2019 to July 2021), vaccination in most pregnant women is likely to have been voluntary without awareness of pregnancy status. The vaccinated subjects may have received only the first dose or both the first and second doses; however, in this study, these two cases could not be distinguished due to data limitations.
To the best of our knowledge, this is the first study to describe a detailed relationship between COVID-19 and obstetric outcomes in pregnant women and neonates based on the population data of Korean women. We found that the rates of preterm birth and cesarean section were significantly lower in women with COVID-19 than in women without infection. In addition, the rates of low birth weight, macrosomia, and NICU admission were comparable between infants born with and without maternal COVID-19 infection. However, since our study had several limitations, additional studies are needed to increase our understanding of the results. It is necessary to continuously monitor pregnant women and newborns who are vulnerable to COVID-19 through the establishment and periodic analysis of cohorts, including maternal factors related to the prognosis of pregnant women and newborns. We also found that an mRNA-based vaccine was less likely to be associated with adverse obstetric outcomes in pregnant women. The data we provide in this study may be useful in guiding the obstetric care of pregnant women during the COVID-19 pandemic.






")











