




Introduction
Cervical cancer is the fourth most common cancer and the leading cause of cancer-related deaths among women worldwide [1]. Cervical cancer screening is one of the most effective types of cancer screening, as evidenced by a substantial decline in both the incidence and mortality associated with it, since the formal publication of the validated Papanicolaou (Pap) smear in 1943 [2,3]. During the 1990s, human papillomavirus (HPV), a sexually transmitted viral infection, emerged as the most important risk factor for the development of preinvasive and invasive cervical cancer [4]. As such, the improved ability to identify and understand HPV has had a tremendous effect for the development of prevention and screening strategies for cervical cancer. HPV vaccines have been developed for carcinogenic and high-risk HPV. Moreover, HPV testing has been added as a component of cervical cancer screening to be used alone or as an adjunctive test to increase the sensitivity for detecting preinvasive and invasive cervical cancer [5-8]. Recent guidelines recommend that women with abnormal cervical cancer screening should be managed according to each patientŌĆÖs estimated risk of high-grade squamous intraepithelial lesion (HSIL) histology or cervical cancer [9-11]. The risk is estimated based on all available screening test results.
In many countries, cervical cytology alone is still the most widely used method for cervical cancer screening [4]. HPV testing in high-grade cytology is considered less important. However, among women with low-grade cytology (i.e., atypical squamous cells of undetermined significance [ASCUS] and low-grade squamous intraepithelial lesion [LSIL]), reflex HPV testing may be beneficial for triaging patients to immediate colposcopy or more conservative wait-and-see surveillance. The American Society for Colposcopy and Cervical Pathology (ASCCP) guidelines recommend reflex HPV testing in ASCUS because HPV testing identifies approximately 90% of ASCUS cases diagnosed with HSIL histology. Furthermore, up to two-thirds of women with ASCUS were negative for high-risk HPV infection, which means that women with a low risk for HSIL histology or cancer may not require colposcopy. As a result, reflex HPV testing in ASCUS can lower the colposcopy rate by half [12,13]. In contrast, in LSIL cytology, the immediate risk for HSIL histology or cancer is below the threshold for immediate colposcopy only if high-risk HPV tests are negative. Because of the higher prevalence (81-83%) of carcinogenic HPV infection in LSIL, reflex HPV testing does not lower the colposcopy rate as much as ASCUS [14-17]. Consequently, the ASCCP guidelines do not recommend HPV triage for LSIL cytology. However, the ASCCP guidelines are based on data collected only from American women. Since there might be geographic variations in both HPV genotype distribution and the risk conferred by each genotype to high-grade lesions or cancer, local management guidelines should be developed based on local HPV epidemiology. Therefore, it is essential for each region to investigate and understand its own specific HPV genotype prevalence and to understand which prevalent HPV genotypes influence significant clinical effects on women living in that region.
The aim of this study was to investigate HPV genotype distribution in LSIL cytology and the immediate risk of cervical intraepithelial neoplasia grade 2 or higher (CIN2+) lesions caused by the corresponding HPV genotype. Knowing the HPV status and its clinical significance relative to the increased risk of CIN2+ lesions may be useful for determining the role of HPV triage in cytology-based cervical cancer screening based on local HPV epidemiology. Furthermore, HPV genotype prevalence can provide important data for targeting the carcinogenic HPV genotypes during HPV vaccine production.
Materials and methods
1. Ethics statement
The study protocol was approved by the Siriraj Institutional Review Board (SIRB) of the Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand (COA No. Si 060/2017). All study participants provided written informed consent prior to enrollment.
2. Study design and study participants
This prospective cross-sectional study was conducted at Siriraj Hospital, ThailandŌĆÖs largest university-based national tertiary referral center. In our center, liquid-based cervical cytology is the most commonly used cervical cancer screening technique. It is our practice to recommend colposcopies for all women with LSIL cytology. Women aged 21 years or older with LSIL cervical cytology who attended our colposcopy clinic between February 7, 2017 and February 7, 2019, were invited to enroll in this study before colposcopy was performed. Pregnant patients and those diagnosed with cervical cancer were excluded.
3. Specimen collection
HPV genotyping was performed at our colposcopy clinic prior to colposcopy assessment. Cervical samples were evaluated using an Anyplex II HPV HR Detection Kit (Seegene, Seoul, Korea) according to the manufacturerŌĆÖs instructions. Multiplex real-time polymerase chain reaction design using tagging oligonucleotide cleavage and extension technology allowed the simultaneous detection and genotyping of 14 high-risk HPV genotypes (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68) and an internal control (human beta-globin) in a single reaction. Colposcopy-directed biopsy was performed during colposcopy in all study participants. In cases where no abnormal cervical lesions were detected, random biopsy was performed. Endocervical sampling was not a mandatory component of this study and was performed in cases of inadequate transformation zone, inadequate colposcopy, or endocervical involvement. Colposcopy procedures were performed under the supervision of experienced colposcopists or gynecologic oncologists. Further management was performed according to local guidelines. The normal protocol at our center is to repeat cervical cytology at 1 year in patients with LSIL cytology with low-grade histology and immediate cervical ablation or conization in patients with high-grade histology with LSIL cytology.
4. Data collection
Prospectively collected data included baseline characteristics, prior cervical cancer screening results, HPV genotyping, colposcopic findings, and cervical histopathology. During the study period, a 2-tiered terminology system was employed (histologic LSIL or HSIL) to report on cervical histopathology according to the Lower Anogenital Squamous Terminology (LAST) Project recommendation [18].
5. Statistical analysis
Continuous variables were presented as mean┬▒standard deviation for normally distributed data, and median and interquartile range were used to describe non-normally distributed data. Categorical variables were presented as frequencies and percentages. Simple proportions were used to establish the risk of CIN2+ lesion values using standard methods to generate a 95% confidence interval (CI). A chi-square test was performed to explore differences in proportions. In cases where at least one cell had a frequency of 5 or less, FisherŌĆÖs exact test was used. This study further explored the differences in the detection of CIN2+ lesions and the number of colposcopies if different types of reflex HPV testing were used. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and overall accuracy were calculated and reported with their respective 95% CIs. The diagnostic performance was compared between tests using McNemarŌĆÖs exact probability test. A P-value <0.05 was considered to be statistically significant for all tests. Statistical analyses were performed using PASW Statistics version 23 (IBM Corp., Armonk, NY, USA).
Results
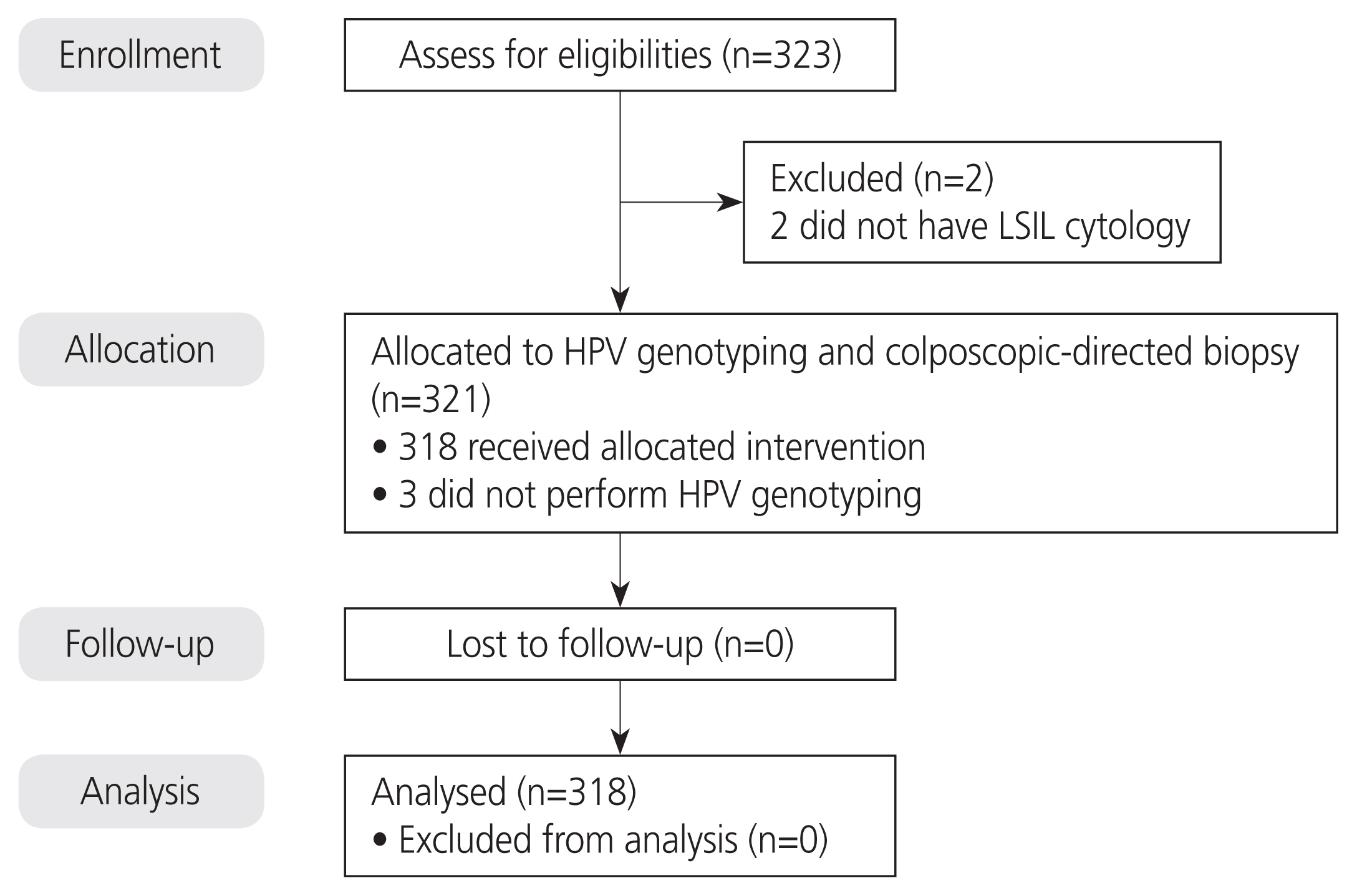
A total of 323 patients with LSIL were identified, but five patients were excluded from the study (Fig. 1). Of these five patients, two did not have LSIL cytology and three did not undergo HPV genotyping. The demographic and clinical characteristics of the women in our study are summarized in Table 1. The mean age of the patients was 39.2┬▒10.3 years, and approximately 81.4% of patients were 30 years old or older. Only 10.7% of the patients were menopausal. Less than half of the patients (48.1%) had no cervical cancer screening or an unknown screening result within the preceding 5 years. Among the 165 patients with available screening results, 83 had normal and 82 had abnormal screening results. Only two patients (0.6%) had a prior diagnosis of CIN2+ lesions.
All patients underwent colposcopy and cervical biopsy. An adequate transformation zone was observed in 252 (79.2%) patients. Normal colposcopic findings, low-grade lesions, and high-grade lesions were observed in 162 (50.9%), 135 (42.5%), and 21 (6.6%) patients, respectively. The number of cervical biopsies ranged from one to four. Endocervical curettage was performed in 41 patients (12.9%), and no CIN2+ lesions were found in the endocervical samples. Histologically confirmed CIN2+ lesions were reported in 6% (19/318) of the patients. One of the 19 patients, who was 46 years old, had adenocarcinoma of the cervix, which was detected using a loop electrosurgical excision procedure (LEEP). Screening performed within the preceding 5 years revealed high-risk HPV-positive (non-16/18) and ASCUS. Recent screening showed HPV18 positivity and LSIL. A colposcopy-directed biopsy revealed adenocarcinoma in situ.
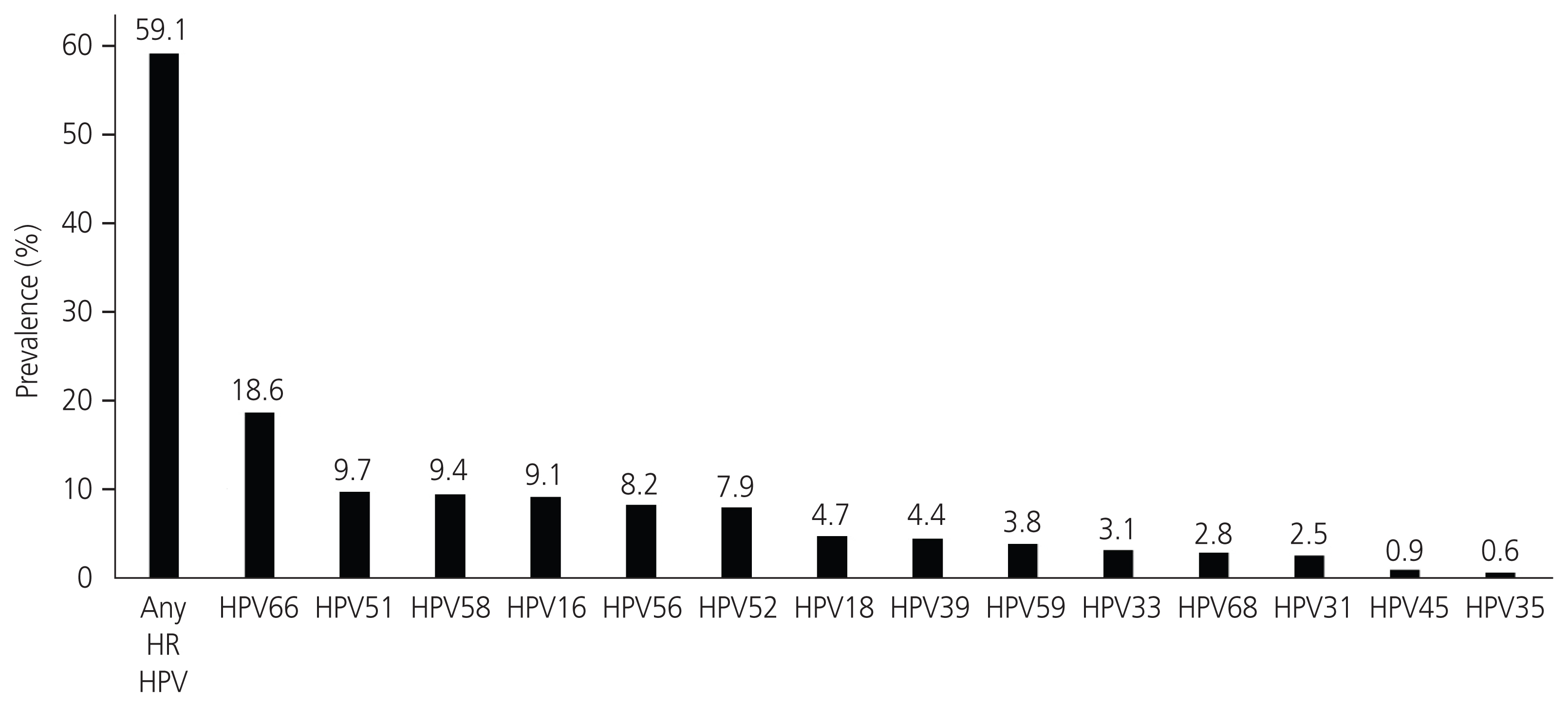
The prevalence of any of the 14 high-risk HPV infections in this LSIL cohort was 59.1% (188/318). HPV66 was the most commonly identified genotype (18.6%), followed by HPV51 (9.7%), HPV58 (9.4%), HPV16 (9.1%), HPV56 (8.2%), HPV52 (7.9%), HPV18 (4.7%), HPV39 (4.4%), HPV59 (3.8%), HPV33 (3.1%), HPV68 (2.8%), HPV31 (2.5%), HPV45 (0.9%), and HPV35 (0.6%) (Fig. 2). A single high-risk HPV infection was observed in 127 patients (39.9%), whereas 61 (19.2%) had multiple high-risk HPV infections (Table 1).
The immediate risk of CIN2+ lesions, according to the HPV status of patients with LSIL, is shown in Table 2. In patients with LSIL, regardless of the HPV status, the immediate CIN2+ risk was estimated to be 6% (95% CI, 3.6-9.2). The immediate CIN2+ risk was 8% (95% CI, 4.5-12.8) in those positive for any of the 14 high-risk HPV genotypes, and 3.1% (95% CI, 0.8-7.7) in those negative for all 14 high-risk HPV genotypes. The immediate CIN2+ risks were 20.7% (95% CI, 8-39.7) in HPV16-positive, 13.3% (95% CI, 1.7-10.5) in HPV18-positive, 16.7% (95% CI, 7-31.4) in HPV16/18-positive, and 5.5% (95% CI, 2.4-10.5) in high-risk non-HPV16/18-positive patients. The immediate CIN2+ risk of HPV66 positivity, which is the most prevalent HPV genotype in this study, was 5.1% (95% CI, 1.1-14.1). It is important to recognize that the estimated risk of CIN2+ is limited in women with multiple HPV infections.
The threshold risk for CIN2+ lesions has not yet been conclusively defined and established; however, the ASCCP guidelines recommend immediate colposcopy in those at or above the threshold for HPV-positive ASCUS or LSIL regardless of HPV their status [10,19]. In our cohort, the immediate risk of CIN2+ lesions in LSIL was 6.0%. If an immediate risk of CIN2+ lesions of 6% is considered to be the clinical action threshold for colposcopy, patients with a risk of Ōēź6% should undergo colposcopy. Table 3 shows a comparison of the diagnostic performance in the detection of CIN2+ lesions and the number of colposcopies among different HPV tests used if 6% was the clinical action threshold for colposcopy. Therefore, colposcopy rates were statistically significantly different in 59.1% (188/318), 13.2% (42/318), and 44.7% (142/318) of patients if reflex HPV testing (reported as negative or positive for any of the 14 high-risk HPV), partial HPV genotyping (reported as negative 14 high-risk HPV, positive HPV16/18, or positive non-HPV16/18), and HPV genotyping (reported as a specific genotype) were used, respectively (P<0.001). The overall accuracy for the detection of CIN2+ lesions was reported as the area under the receiver operating characteristic curve (Table 3). The analysis revealed no significant difference among the three tests: 0.6 for HPV testing, 0.53 for partial HPV genotyping, and 0.46 for HPV genotyping (P=0.149). The estimated sensitivity, specificity, PPV, and NPV, according to the type of HPV testing, are shown in Table 3.
There were no significant differences in age, menopausal status, history of abnormal screening, or number of high-risk HPV infections between women with LSIL and HSIL histology (Table 4). Colposcopic findings were significantly associated with HSIL histology (P=0.028) and revealed that HPV infection was significantly more common in HSIL histology than in LSIL cytology (78.9% vs. 57.9%, P=0.097). However, combining the colposcopic impression with HPV status was significantly associated with HSIL pathology (P<0.001).
Discussion
The prevalence of high-risk HPV infection in this this hospital-based Thai cohort was 59.1%. The five most common genotypes were reported to be HPV66 (18.6%), HPV51 (9.7%), HPV58 (9.4%), HPV16 (9.1%), and HPV56 (8.2%). The prevalence of high-risk HPV infection in this cohort was relatively low compared to that in previous reports from other countries/centers/studies: Korea (69.0%), China (70.8%), Brazil (76.0%), Kaiser Permanente Northern California (KPNC) (81.0%), ASC-US/LSIL Triage Study (83.0%), and the United Kingdom (83.9%) [20-25]. Concerning other studies reported from Thailand, LSIL with high-risk HPV infection was much more prevalent in Northern and Northeastern Thailand (74.8-93.3%) [26-28] compared with the rates observed in Central Thailand (46.7-54.8%) [29,30]. Furthermore, the most common HPV genotype in our study was HPV66, which differs from previous studies that reported HPV16 to be the most prevalent genotype [21,24,25,31]. In regions where high-risk non-HPV16/18 is common, a nonavalent HPV vaccine should be recommended rather than a quadrivalent one. Differences in the geographic and ethnic distributions of HPV genotypes were first proposed by Bruni et al. [32] in 2010. Other explanations that may help explain these differences in findings include variations in HPV testing techniques, HPV vaccine coverage, and source of study data (hospital-based or population-based study). The observed and reported geographic variations in HPV genotypes support the idea that management guidelines should be developed based on the regional HPV epidemiology.
The 2019 ASCCP risk-based management consensus guidelines for abnormal cervical cancer screening tests and cancer precursors proposed the principle of risk-based management [9-11]. These guidelines recommend that the clinical action threshold for surveillance, immediate colposcopy, or expedited treatment should be based on each individual patientŌĆÖs risk for CIN3+ lesions, in addition to the results of current and prior screening. If the immediate risk of CIN3+ is greater than or equal to 4%, immediate colposcopy is recommended. The immediate risk of CIN3+ as per the 2019 ASCCP guidelines was 1.1% in high-risk HPV-negative LSIL (surveillance recommended) and 4.3% in high-risk HPV-positive LSIL (colposcopy recommended) [9,10]. However, the immediate risk thresholds for CIN3+ were generated from the data of patients treated at centers associated with Kaiser Permanente, Northern California, USA. Thus, the generalizability of these recommendations for other populations should be further investigated.
The present study was conducted to evaluate the immediate risk of high-grade cervical lesions in the Thai LSIL population based on the HPV genotype. Although the ASCCP guideline uses CIN3 as a definition of precancer, our study used 2-tier terminology (histologic LSIL or HSIL) during the study period [10]. Therefore, CIN2 was defined as the endpoint of precancer in our study. In our cohort, the immediate risk of CIN2+ was 6% (95% CI, 3.6-9.2), 8% (95% CI, 4.5-12.8), and 3.1% (95% CI, 0.8-7.7) in LSIL, HPV-positive LSIL, and HPV-negative LSIL, respectively (Table 2). In contrast, the KPNC study during 2003-2010 reported the immediate risk of CIN2+ to be 8.7%, 10.0%, and 2.1% in LSIL with unknown HPV status, HPV-positive LSIL, and HPV-negative LSIL, respectively [22,23]. The risk of CIN2+ was lower in our LSIL cohort than that in the KPNC cohort. This might be due to the fact that the most common HPV genotype found in our study was HPV66 (20.7%) and not HPV16, which is the most highly carcinogenic HPV genotype. Our result is also inconsistent with prior studies that reported HPV16 as the most common genotype found in LSIL [24-30].
Since the immediate risk of CIN2+ in LSIL, regardless of HPV status, was used as a threshold for colposcopy, 6% was the risk cut-off. All types of HPV testing combined with LSIL cytology showed a significant decrease in colposcopy ratesŌĆö decreased by 86.8% in partial HPV genotyping, 55.3% in HPV genotyping, and 40.9% in HPV testing when these tests were combined with LSIL cytology findings. Only HPV testing had an overall accuracy that met the accepted AuROC value of 0.6. Furthermore, HPV testing provided the highest NPV, which was useful for triaging patients with LSIL for colposcopy or surveillance. However, our finding-based recommendations do not coincide with those from the ASCCP guideline, which do not support performing reflex HPV testing in LSIL. This may be because of the greater prevalence of high-risk HPV and more carcinogenic genotypes, like HPV16, have been found in a USA-based population with LSIL [10,19,23]. These studies suggest that reflex HPV testing might not be as helpful in reducing the number of colposcopies in the USA population. The decision to add reflex HPV testing in patients with LSIL cytology should consider multiple factors, including genotype distribution, the clinical significance of prevalent HPV genotypes, local infrastructure, test availability, and cost-effectiveness.
The present study found no clinical factors that significantly predicted CIN2+ lesions in LSIL cytology, except for colposcopic findings alone or colposcopic findings combined with HPV status. However, in real-life clinical practice, colposcopic findings cannot be used as a prognostic tool to guide colposcopy performance. Prior studies have reported that high-risk HPV infection could help predict CIN2+ in low-grade cytology, but that previous or baseline patient characteristics could not [33-35].
However, this study has some limitations. First, the follow-up duration was relatively short. A study with a longer duration of follow-up might further clarify the cumulative risk of CIN2+ and help determine the optimal interval of surveillance. Second, CIN2 was used as an endpoint for precancer in our study. This is a drawback since CIN2 is less reproducible, less prognostic, and resolves spontaneously compared to CIN3 [36,37]. The current guidelines supports differentiating CIN2 from CIN3 within the HSIL group because this can influence clinical decision-making (i.e., conservative management, risk estimation, and surveillance) [10,38]. Finally, some low prevalence HPV genotypes were found with wide confidence intervals. Therefore, the estimated risk of CIN2+ lesions in these genotypes should be considered to be less precise. The development and implementation of screening guidelines requires data from a large nationwide population-based study with long-term follow-up data. A cost-effective analysis would also be beneficial for hospital administrators and healthcare policymakers.
In conclusion, the results of this study highlight the association of geographic variations with HPV genotypes. It suggests that population-specific guidelines should be established based on epidemiology and clinical characteristics. Reflex HPV testing may decrease the number of colposcopies in countries with a high prevalence of low carcinogenic HPV, based on cytology-based screening.






")











