



Introduction
In placentation of normal pregnancies, the spiral arteries are invaded by endovascular trophoblast, resulting in extensive remodeling of these arteries. Because of this change, the uterine artery Doppler in normal pregnancies is characterized by low resistance and a high-flow pattern. However, in hypertensive pregnancies, incomplete trophoblast invasion results in an abnormal uterine artery Doppler pattern, which is characterized by an increased pulsatility index (PI) and an early diastolic notch [1,2,3,4].
Based on the pathophysiology, it has been reported that abnormal uterine artery Doppler in hypertensive pregnancies is associated with adverse perinatal outcomes, such as early delivery and low birthweight [5,6,7,8,9]. Moreover, it has also been reported that the increased PI of the uterine arteries in the 1st trimester may be used in prediction of hypertension and small for gestational age [10,11,12,13,14,15,16,17,18].
Delivery is thought to be the definitive treatment of hypertensive disease in pregnancy, because the placenta is removed and maternal hypertension is resolved in the postpartum period. However, whether or not increased uterine impedance is resolved after delivery is unclear.
In the puerperal period, uterine involution involves not only uterine muscle and endometrium but also the uterine arteries and branches, resulting in dynamic changes of uterine artery Doppler. There have been several reports on the postpartum changes of uterine artery Doppler in normal pregnancies [19,20,21,22,23,24,25,26]. In most of these studies, uterine artery indices such as the resistance and pulsatility indices increased during the postpartum period [19,20,22,23,24,26], although some could not find significant changes during the postpartum period [21,25]. However, there is a paucity of information regarding the postpartum uterine artery Doppler in hypertensive pregnancies.
The objective of this study was to investigate whether the uterine artery pulsatility index (UtA PI) of hypertensive pregnancies is higher than that of normal pregnancies in the postpartum period as in the antepartum period.
Materials and methods
1. Study design
In this cross-sectional study, we measured the UtA PI in singleton pregnancies during the antepartum, immediate postpartum, and late postpartum periods. Each woman underwent Doppler examination once among these three periods. Antepartum measurement was performed at 24 to 40 weeks gestation, and immediate postpartum measurement was performed several days after delivery (usually 2 days). Late postpartum measurement was performed several weeks after delivery (usually 3 to 5 weeks). The institutional review board of Seoul National University Hospital approved this study, and patients gave their written consent for the collection of data for research purpose.
Cases were divided into 2 groups according to the presence or absence of hypertensive disease in pregnancy: group 1, women with hypertensive disease in pregnancy, including gestational hypertension, preeclampsia, eclampsia, chronic hypertension or superimposed preeclampsia; group 2, women with normotensive pregnancies.
2. Doppler measurement of the uterine arteries
Ultrasound examinations of the bilateral uterine arteries were performed by the transvaginal approach, using an Accuvix XQ (Medison, Seoul, Korea). The participants were asked to empty the bladder before the examinations and placed in the dorsal lithotomy position. The main uterine artery was identified at the level of the internal cervical os with color Doppler, and then pulsed Doppler was used to obtain the mean value of three consecutive data of the UtA PI. The same process was repeated for the contralateral uterine artery. The mean value of the bilateral uterine arteries was used for data analysis. The presence or absence of early diastolic notches was also documented. In women during the antepartum period, a Doppler examination of the fetal umbilical artery was also performed. All measurements were performed by a single examiner (LSM).
3. Statistical analysis
Statistical analyses were performed using SPSS ver. 12.0.1 (SPSS Inc., Chicago, IL, USA). Comparisons of continuous variables between groups were performed with the Mann-Whitney U-test. Proportions were compared with the FisherŌĆÖs exact test. A P-value of <0.05 was considered significant.
Results
1. Characteristics of the study population
One hundred twenty-two women were enrolled: group 1, women with hypertensive disease in pregnancy (11 cases in the antepartum period, 13 cases in the immediate postpartum period, and 10 cases in the late postpartum period); group 2, women with normal pregnancies (32 cases in the antepartum period, 29 cases in the immediate postpartum period, and 27 cases in the late postpartum period). Cases with fetal anomalies, intrauterine growth restriction without hypertensive disease, other obstetric or medical diseases that can affect the uterine circulation (including diabetes, autoimmune diseases, or uterine malformations) and placenta previa were excluded.
Table 1 shows the clinical characteristics of the study population. In the antepartum period, there were no significant differences in maternal age, parity, gestational age at the time of measurement, estimated fetal weight, and amniotic fluid index. However cases in group 1 had a higher UtA PI, an earlier gestational age at delivery, and a smaller birthweight than cases in group 2.
In the immediate and late postpartum periods, there were no significant differences in maternal age, parity, postpartum measurement days, and uterine size at the time of measurement between the two groups. However, cases in group 1 had an earlier gestational age at delivery and a smaller birthweight than cases in group 2.
2. Doppler measurements of the uterine arteries
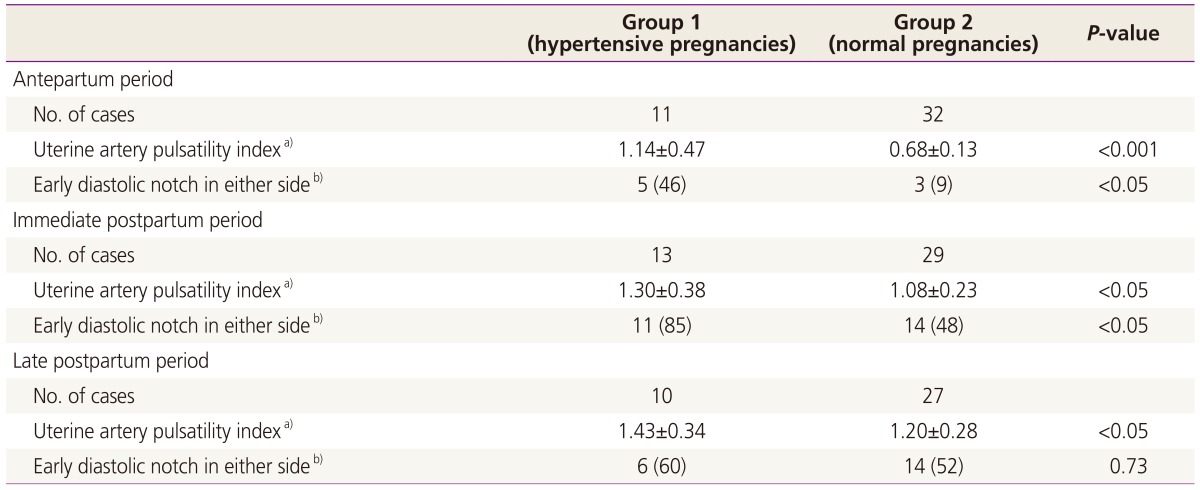
In the antepartum and immediate postpartum periods, the mean value of UtA PI in group 1 was higher than in group 2 (Table 2). The proportion of cases with an early diastolic notch in at least one side was higher in group 1 than that in group 2 (antepartum period mean UtA PI, 1.14 in group 1 vs. 0.68 in group 2, P<0.001; percentage of early diastolic notch, 46% vs. 9%, P<0.05; immediate postpartum period mean UtA PI, 1.30 vs. 1.08, P<0.05; percentage of early diastolic notch, 85% vs. 48%, P<0.05).
The mean value of UtA PI in group 1 in the late postpartum period was also higher than that in group 2. The proportion of cases with an early uterine artery notch was higher in group 1 than that in group 2, but this difference did not reach statistical significance (mean UtA PI, 1.43 vs. 1.20, P<0.05; percentage of early diastolic notch, 60% vs. 52%, P=0.73).
Discussion
The principal finding of our study is that the mean value of UtA PI of hypertensive pregnancies was still higher than that of normal pregnancies in the immediate and late puerperal period, as well as in the antepartum period.
In hypertensive pregnancies, blood pressure is normalized and proteinuria disappears within several days after delivery. Does clinical improvement coincide with resolution of underlying basic pathophysiologic change? We adopt a uterine artery Doppler as an indirect method to identify it, and showed that the uterine artery impedance did not resolve, even several weeks after the delivery of the placenta.
Several mechanisms can be offered for this finding. First, the increased uterine artery impedance may be the result of remaining defective trophoblast invasion in the area of the basal zone of the decidua basalis (zona basalis) and myometrium, which remains even after delivery of the placenta [27]. Second, atherosis within the spiral arterioles can remain in the placental bed, to which the decreased placental perfusion has been also attributed [28,29,30,31]. Third, persistently increased maternal vascular tone could affect uterine arterial impedance. The last explanation is unlikely, because the persistence of maternal hypertension in the postpartum period was not associated with increased UtA PI in our data. In immediate postpartum period, 69 % (9/13) of women in group 1 had persistent hypertension, but the mean value of UtA PI was not different between women with persistent hypertension and those with resolved hypertension (UtA PI, 1.41 in women with persistent hypertension vs. 1.05 in women with resolved hypertension, P=0.15). In late postpartum period, 30 % (3/10) of women in group 1 had persistent hypertension, but the mean value of UtA PI was not different between women with persistent hypertension and those with resolved hypertension (UtA PI, 1.34 vs. 1.47, P=1.0). Fourth, different antepartum uterine artery indices between normotensive women and hypertensive women can result in different postpartum uterine artery indices, even after similar postpartum changes in uterine artery.
The antepartum mean UtA PI in group 1 was 1.14 measured at a mean gestational age of 33.8 weeks. The reported 95th percentile value of uterine artery PI at 34 weeks of gestation was 1.185 [32]. This means that the mean value of uterine artery PI was around the upper cut-off values of normal range. Another study also reported the mean values of UtA PI within normal range even in hypertensive group [33].
In the current study, we used transvaginal probe for measurement of uterine artery indices. Because trans-abdominal approach is not practical in postpartum, we adopted a transvaginal approach method to standardize the measurement technique during the antepartum and postpartum periods. The reliability of transvaginal measurement of uterine artery Doppler in the antepartum period was reported by several investigators [34,35].
Recently, the study about postpartum uterine artery Doppler velocimetry among patients with preeclampsia and the study about uterine artery impedance during puerperium in chronic hypertensive pregnancies were reported [33,36]. We included not only preeclampsia but also other hypertensive diseases such as gestational hypertension, chronic hypertension and superimposed preeclampsia in group 1. Increased uterine artery impedance is observed not only in preeclampsia but also other hypertensive diseases in pregnancy, because the defective trophoblast invasion, which is thought to be the main mechanism of uteroplacental insufficiency, could be identified in hypertensive diseases other than preeclampsia [4,37].
We demonstrate that the mean value of UtA PI in hypertensive women was still higher than that in normotensive women even in the late postpartum period, and the mean of postpartum day at measurement in the late postpartum period was 28 days in the current study. A more extended period of follow-up would be needed, considering that it would take more than several weeks for uterine artery indices to return to the non-pregnant state, as shown in studies on the postpartum uterine artery Doppler of normal pregnancies [19,24,26,38,39]. We believe this kind of information would enhance our understanding on vascular changes during postpartum in hypertensive women.
The clinical significance of postpartum uterine artery Doppler measurement needs further studies. The association between postpartum uterine artery Doppler and long-term cardiovascular or neurovascular consequences, or the association between postpartum uterine artery Doppler and other vascular indices such as arterial stiffness can be next research issues.
This study also confirms that in the antepartum and immediate postpartum periods the proportion of cases with early diastolic notch was significantly higher in group 1 than in group 2. But the difference for presence of early diastolic notch between the two groups of cases was disappeared in the late postpartum periods, mainly because of the increasing frequency of early diastolic notch in postpartum period in group 2 (normal pregnancy). The finding that the proportion of cases with early diastolic notch was increasing in normal pregnancy is consistent to the findings of other reports [33,38]. This trend may be based on a process for uterine artery to return to the non-pregnant state.
In conclusion, UtA PI of hypertensive pregnancies was still higher than that of normal pregnancies in the immediate and late puerperal periods. This data suggests that longer period may be needed for the resolution of vascular change than resolution of clinical parameters during postpartum in hypertensive women.







")











