



Introduction
Pelvic organ prolapse (POP) is a significant public health concern in women and is a common indication for gynecological surgery [1-6]. POP is defined as “the descent of one or more aspects of the vagina and uterus: the anterior vaginal wall, posterior vaginal wall, the uterus (cervix), or vaginal vault”. POP causes a huge social and economic burden and adversely affects quality of life. The lifetime risk of POP surgery in women is estimated at 20% [1,7-9]. POP can cause various symptoms such as vaginal bulging, pelvic pressure, sexual dysfunction, lower urinary tract dysfunction, and defecatory dysfunction [2,10-13]. To treat these symptoms, doctors use surgical or non-surgical methods according to the patient’s preference or condition [2,12-16]. In the United States, the prevalence of symptomatic POP is expected to exceed 46% to become 4.9 million women by 2050 [1,14]. In addition, older women show a higher rate of POP, with a 30% risk factor; 180 per 100,000 women aged 50 years or older in South Korea suffer from POP [2,16].
POP was diagnosed based on pelvic examination [2,17]. The International Continence Society recommends using a pelvic organ prolapse quantification (POP-Q) system during pelvic examinations [2,10]. Quantitative measurement by the POP-Q system aids in understanding the affected site and the degree of prolapse. However, it does not identify the underlying supporting defects or differentiate the organs involved (e.g., rectocele vs. enterocele) [2,11]. Imaging studies can help to solve this problem. Since the beginning of the 21st century, magnetic resonance imaging (MRI) and translabial ultrasound (TLUS) dynamics with several adjustments have been used as adjunctive tools for diagnosing POP [2,12,13]. MRI is expensive and has a low availability. TLUS is an easy, cheap, and non-harmful diagnostic method that is appropriate in most gynecologic clinics with pre-existing ultrasonography machines, and involves no additional equipment purchase [2,18].
In this review, our goal was to discuss the clinical advantages of using TLUS to diagnose POP along with a literature review.
Methods
The authors of this review conducted an online literature search for studies conducted among humans from inception to March 2022. Two databases were included in this investigation: Google Scholar and PubMed. There were no language restrictions. The following words and subject terms were used in this search: “enterocele, pelvic organ prolapse, rectocele, and ultrasonography”.
The authors included all studies found, regardless of the nature of the study. The titles and abstracts were reviewed individually. If information was insufficient in the abstracts, the authors then retrieved and assessed the relevant full texts to determine their eligibility.
The use of TLUS in urogynecology
Recently, the use of TLUS in urogynecology, particularly for assessing the female pelvic floor, has progressed significantly, accompanied by the development of ultrasonographic technology with enormous potential to improve women’s health [18-22]. TLUS is an objective and reproducible technique to evaluate the female pelvic floor and significantly improves the comprehension of the relationship between female pelvic floor dysfunction and delivery [18-22].
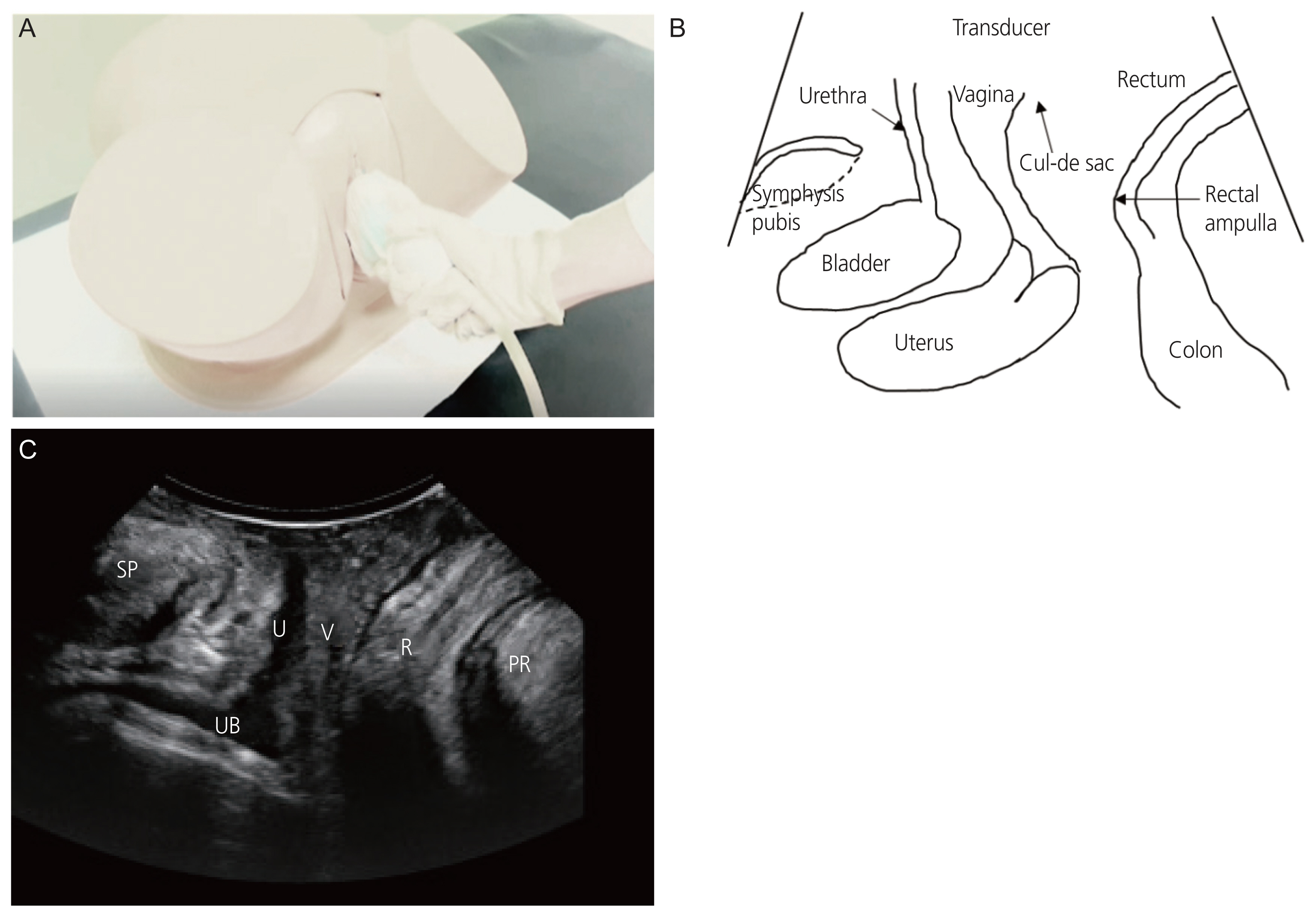
The two-dimensional TLUS can assess the midline structure of the pelvic floor as presened in Fig. 1C [18,23]. The three-dimensional (3D) technique is essential for visualizing the plane of the pelvic floor muscles, including the levator ani muscle (LAM). The LAM is “the main support muscle of the pelvic organs that is fundamental for normal pelvic function”. Because LAM is set in the axial plane, it cannot be observed without 3D ultrasound [18,20,24,25].
To evaluate POP using TLUS, the patient must be in the semi-fowler position with the hips bent and abducted. Using a transabdominal probe, a 3.5-5 MHz convex array transducer can be implemented on the labium major after evacuation before the exam (Fig. 1A). Even after evacuation, some patients still have full bladders because of incomplete evacuation of the cystocele. Doctors should apply a large amount of jelly on both the transducer and probe cover so as not to interfere with the air of the vaginal sulcus. All TLUS measurements should be performed in the relaxing mode and during the maximal Valsalva maneuver. Rectocele or enterocele presence was defined as “the descent of either the rectal ampulla or the small bowel, sigmoid colon, or omentum into the cul-de-sac” (Fig. 1B). The peritoneal cul-de-sac loaded with echogenic small bowel and peristalsis was clear in cases of enterocele during the maximal Valsalva maneuver [22]. Even in patients with procidentia, there can be no rectocele or enterocele, with only posterior vaginal wall relief. Dietz et al. [23] reported that the descending of the cervix, urethra, bladder, and rectum during the Valsalva maneuver is simple to record in the midsagittal plane with a signal to a landmark determined by the inferoposterior margin of the symphysis pubis, with no need for the 3D technology [17,23]. However, in other cases, 3D ultrasound is likely to be helpful in identifying fascial defects such as transverse or lateral ruptures of the rectovaginal septum [17,25]. In addition, 3D datasets allow data storage for further analysis. 3D TLUS increases intra- and inter-observer reproducibility in assessing POP [18].
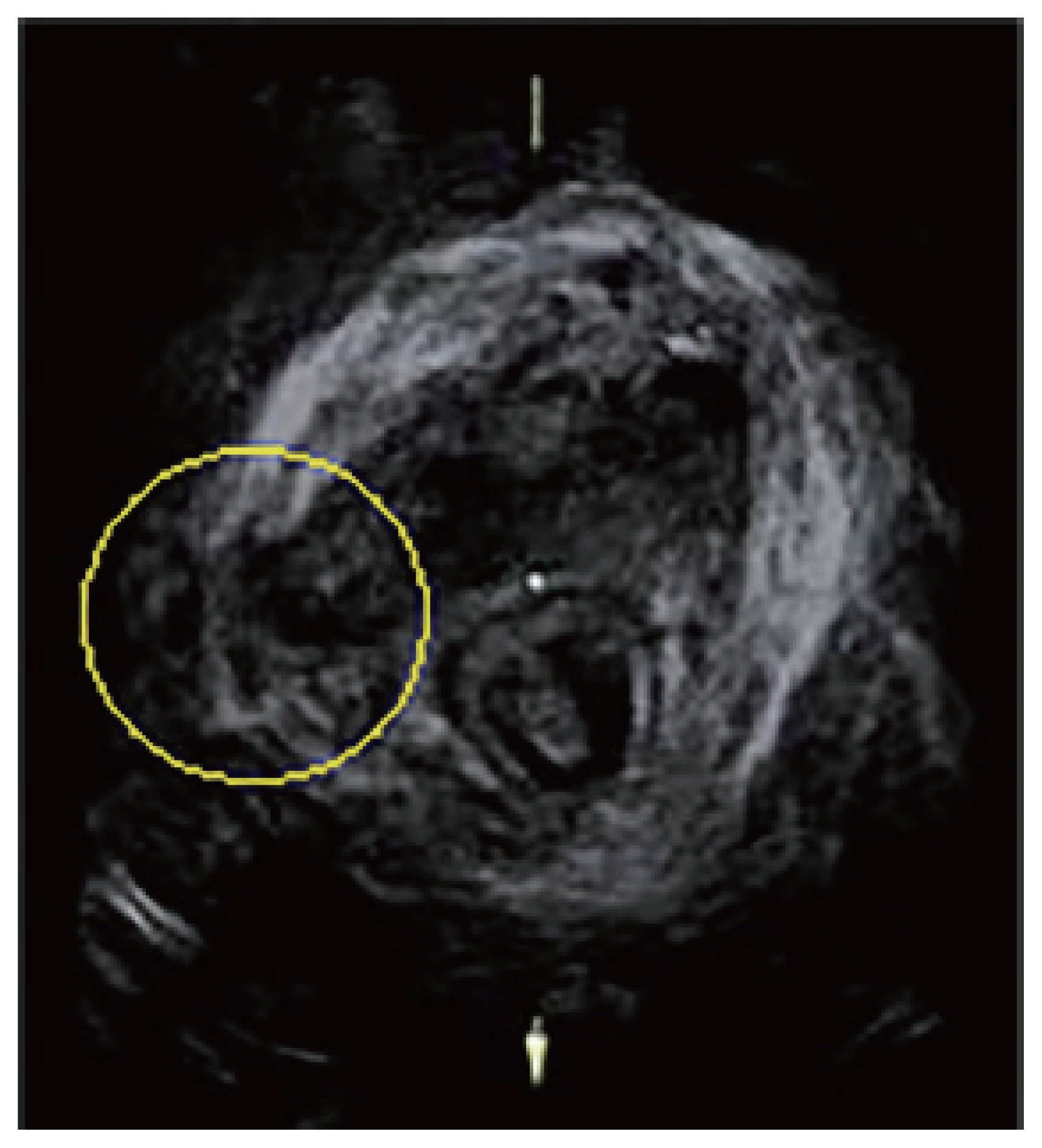
Dietz et al. [26] in 2005 demonstrated 3D TLUS as a reliable and reproducible technique for evaluating LAM biometry, and recognized the biometric parameters of the LAM and levator cavity. They also reported a considerable correlation between the levator cavity area and pelvic organ falling, which affirmed the previous hypothesis that LAM anatomy and integrity play an independent role in determining pelvic organ prolapse. LAM abnormalities are common in urogynecological patients, especially women of childbearing age who have at least one baby, and are correlated with falling of the anterior and apical parts [27]. It is also possible to have “tomographic imaging” with 3D TLUS by tomographic ultrasound imaging (TUI), which reproduces pelvic floor “slices” [18].
3D/4D TLUS is a fast-evolving area with considerable potential to improve women’s health and increase comprehension of the pathophysiology and etiology of female pelvic floor dysfunction [2,18]. Several studies have determined an average-to-almost excellent reproducibility (inter-observer reliability) for measuring levator hiatal dimensions with 3D/4D TLUS under relaxed and moving conditions [28,29]. van Veelen et al. [30] revealed that in women with or without a baby, the use of 3D/4D ultrasound imaging to measure the levator hiatus and levator-urethra gap is very reliable. They stated that the mechanism used to measure levator hiatal measures is simple, while the levator-urethra gap measurement using TUI is more complex [26,28-31]. Another study by van Delft et al. [32,33] compared 3D and 4D TLUS with endovaginal ultrasound and digital palpation to assess pelvic floor muscle contractility. They reported a high correlation among the three methods.
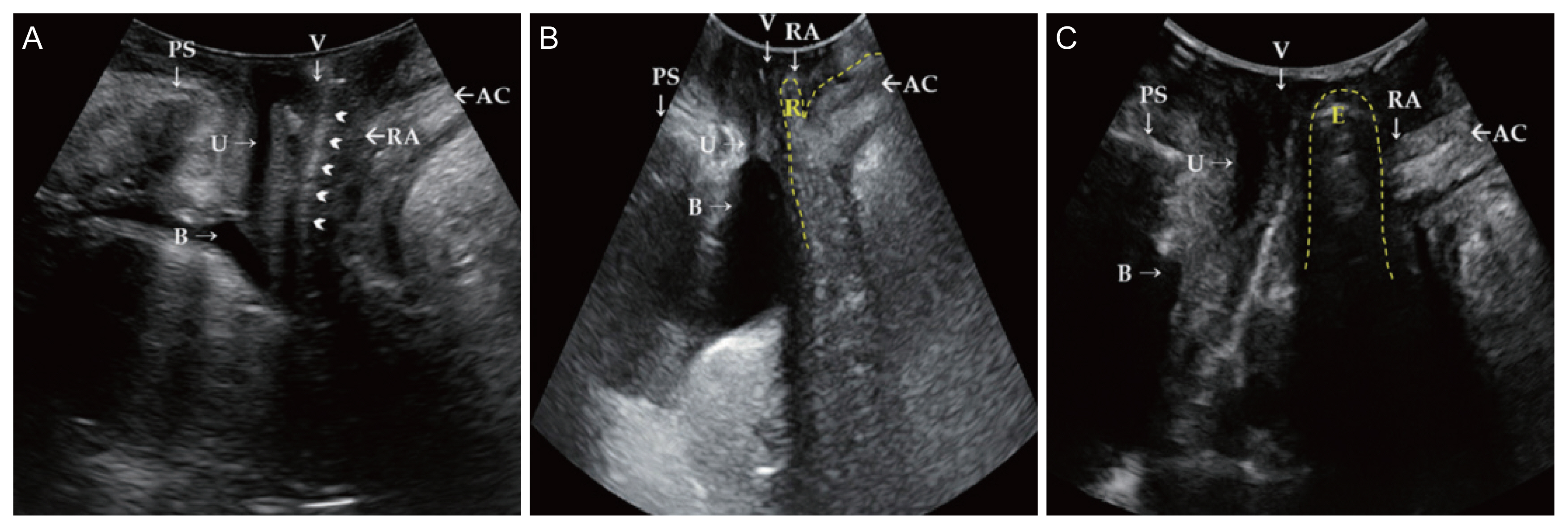
In terms of the role of TLUS as an adjunct to the POP-Q examination to provide an accurate diagnosis of POP, the standard POP-Q examination quantifies all parameters. Six points are placed on the vaginal wall. Then, the space between the hymen and these points is measured using the maximal Valsalva maneuver. The following points should be determined: “two posterior points (Ap and Bp), two anterior points (Aa and Ba), two apical points (C and D), genital hiatus, total vaginal length, and perineal body”. POP-Q 0 to the fourth stage is identified based on the area between the most dependent part of the pelvic organ and the hymenal ring as presented in Figs 2, 3 [2,34]. Although this is a widely used standardized method, it is subjective and cannot precisely identify which organ is in the prolapsed vaginal sac. In addition, several reports have confirmed false POP due to conditions mimicking POP [35-37].
In cases of real POP, particularly in posterior prolapse, it is difficult to determine the existence of rectocele or enterocele with posterior vaginal wall repose only by physical examination, even with POP-Q staging. In uterovaginal prolapse, most doctors anticipate that the rectum or, infrequently, the small bowel is in the sack of the posterior vaginal wall if the POP is completely prolapsed. However, on TLUS, they usually face only a reposed posterior vaginal wall composed of a pouch that does not involve an enterocele or rectocele [2]. Treating plans must be adjusted according to the anatomical state and the presence of rectocele or enterocele [17]. TLUS simplifies the differential diagnosis of a real rectocele or simple posterior vaginal repose. Some researchers have reported that for asymptomatic rectoceles, the combination of posterior reform and surgical reform of apical prolapse minimizes the risk of poor surgical outcomes. However, there is still a debate regarding this surgical plan [38,39]. The necessity for regular posterior reform should be re-evaluated after the differential diagnosis of a real rectocele or simple posterior vaginal repose to decrease the rate of avoidable posterior repair. In cases of POP with an enterocele, doctors should surgically repair the enterocele by excision or ligation of the enterocele pouch. Fixing the rectovaginal septum without enterocele reform may lead to the POP recurring [2].
Correlation of TLUS and POP-Q exam outcomes
Until now, TLUS was mainly used to detect “the ureterocele, cystocele, rectocele, and enterocele,” which could remain undiagnosed, or misdiagnosed, using the POP-Q method. In 2005, Dietz and Steensma [17] stated that TLUS could be used to measure POP linked with the clinical staging of the POP-Q method. The researchers indicated that TLUS could identify POP using a reference line comprising the symphysis pubis inferior margin [2]. Greater descent of the uterus, cul-de-sac, bladder, and rectal ampulla during the Valsalva maneuver was computed [40]. Dietz et al. [23] reported an excellent relationship between ultrasound results and clinical staging of anterior and apical prolapses.
In contrast, Nam et al. [2] reported a weak connection between POP-Q outcomes and TLUS findings, mainly in the posterior part of POP. The POP-Q method showed prolapse of the posterior part and repose of the posterior vaginal wall with no enterocele or rectocele, which was evident on TLUS [2]. Some researchers have stated that using TLUS is an accurate and simple measurement method of the anorectal junction position, either in the rest mode or when it is active during straining [41]. It is difficult to distinguish between true and false rectoceles and detect whether a clinically apparent rectocele is caused by a rectovaginal septum, perineal hypermobility, or an isolated enterocele [17]. The moderate sagittal plane on TLUS can identify real rectocele cases caused by a rectovaginal septum defect [16].
Role of transperineal ultrasound in separating true POP cases from cases mimicking POP
Many conditions characterized by multiple vaginal masses may mimic POP. Braga et al. [42] reported the case of a woman with the main complaint of vaginal bulging and overactive bladder signs with POP-Q stage II anterior vaginal prolapse. Histopathological examination revealed an anterior vaginal leiomyoma. POP can be misdiagnosed in patients with vaginal wall cysts, vulvovaginal hemangioma in Klippel-Trénaunay syndrome, a perineal mass, or long cervical polyps [35,36].
Consequently, imaging techniques have been used to detect pelvic floor deflects and their association with neighboring organs, as an accompaniment to the POP-Q method. Even with the critical information provided by defecation proctography and MRI [2,43], they are seldom used in daily clinical practice, because they are costly, may not be accepted by patients, and carry risks of radiation exposure or allergic reactions to the contrast media. TLUS is more widely utilized because it is a commonly used, user-friendly imaging modality that is cheaper, easier to perform, and quicker, taking approximately 5 minutes. It provides the same information as the other two techniques [2,18]. The urogynecologist can implement surgical procedures for POP patients without performing defecation proctography and MRI. TLUS can enhance the accuracy of POP diagnosis when combined with a POP-Q exam with minimal extra effort and cost.
Conclusion
TLUS is an easy, inexpensive, and non-harmful diagnostic method that is appropriate for most gynecologic clinics.
TLUS is valuable in POP diagnosis, as it plays a role in recognizing POP cases and separating them from cases mimicking POP. There is a debate about the relationship between the POP-Q exam and TLUS. Particularly for posterior compartment POP. TLUS should be performed for patients with POP-Q exam results indicating a posterior compartment POP, to determine the existence of enterocele or rectocele. Further studies on the TLUS technique and its use in urogynaecology are needed to improve women’s health.






")











