



Introduction
Cervical cancer continues to be one of the most common cancers among women globally [1]. The main causative agent of cervical cancer is persistent infection with oncogenic human papillomavirus (HPV) at the cervix, which results in intraepithelial lesions, defined histologically as cervical intraepithelial neoplasia (CIN) lesions. Low-grade lesions include CIN1, which is a morphological expression of HPV infection. High-grade lesions include CIN2, which is considered a mixture of CIN1 and CIN3 and has a higher frequency of regression, and CIN3, which progresses to invasion in 9 years [2,3]. Progression to intraepithelial pre-cancers involves the disruption of the HPV virus cell cycle control pathways mediated by overexpression of the viral E6 and E7 proteins that, among other actions, functionally inactivate the products of the retinoblastoma and p53 immunosuppressive genes. The overall process is complex and includes a number of genetic and epigenetic alterations [4,5]. The specificity of high-risk HPV DNA testing is too low to be useful for the diagnosis of low-grade lesions (23% for atypical squamous cells of undetermined significance and 17% for low-grade squamous intraepithelial lesions [LSILs]) [6,7]. A potential biomarker with high specificity values is required to avoid over-diagnosis and potential overtreatment in this category of patients.
MicroRNAs (miRNAs) are an abundant class of small, non-coding RNA genes that comprise short sequences of nucleotides (approximately 22 nucleotides) that control post-transcriptional regulation of gene expression [8]. Accumulating evidence on miRNA profiles in carcinogenesis has demonstrated their strong ability to differentiate various cancers and their tumor stages [9,10]. Analysis of miRNA functions has established that miRNAs play a crucial role in many physiological processes and developmental health [11]. In turn, miRNA expression levels are altered in many diseases, especially human cancers [12]. Various miRNAs have been identified in many cancers, including hepatocellular cancer, pancreatic cancer, stomach adenocarcinomas, ovarian cancer, breast cancer, and cervical cancer [12].
However, the exact role of miRNAs in cervical carcinogenesis is still largely unknown, especially in non-conventional sampling materials such as cervical mucus and plasma serum [13]. We systematically reviewed the literature to evaluate the role of miRNAs as biomarkers in the progression of cervical precancerous and cancerous lesions.
Methods
A systematic literature search was conducted using electronic databases for studies published between January 2010 and June 2020. The databases used included PubMed, Science-Direct, Embase, and Cochrane Controlled Register of Trials. Boolean operators and text words were combined to create the following keywords: “microRNA” and “cervical” and “lesion.” Reference lists of selected studies and review articles were examined to ensure that no relevant studies were omitted. Table 1 lists the search queries used and the number of articles obtained from each electronic database. To ensure that the studies included were eligible for subsequent review, specific criteria were used to distinguish relevant studies from all the initial studies found. The selected studies fulfilled the inclusion criteria detailed in the next sector.
Study selection
Two authors (K.N. and E.B.) independently screened the title and abstract of each record retrieved to identify potentially relevant articles for full-text review. If the two reviewers did not agree, a third reviewer arbitrated. Inclusion criteria included all study designs that aimed to evaluate correlations between miRNA expression and different precancerous cervical stages and/or cervical cancer were included except case reports and case series. All meta-analyses; systematic reviews; randomized and nonrandomized clinical trials; retrospective and prospective observational studies; phase I, II, and III clinical trials with study samples consisting of cervical cells, cervical tissues, serum, mucus, or a combination of these were included. The exclusion criteria included narrative reviews, letters, editorials, commentaries, case studies, case series, non-human studies, non-cervical cancer cases, studies experimenting only on cell lines, miRNAs that were investigated only in advanced cervical cancers or lymph node metastasis, studies on miRNA-related polymorphisms, and studies not published in English. The selected articles were discussed among the investigators during the screening phase. The selection process included three main processes: (1) identification of records, (2) screening of records, and (3) assessing eligibility of records and were presented accordingly in a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart.
Data extraction and synthesis
Two authors (K.H. and M. F.) independently extracted the data from the included studies in a piloted data extraction form. The data extracted from individual studies included information on the title, study design, first author, publication year, publication journal, sample size, sample type, country of study, age group of participants, discovery and quantification methods of miRNAs, internal reference gene used for normalization, miRNAs significantly expressed in different types of samples, miRNA expression profiles (upregulated or downregulated) in various cervical disease states, HPV-related findings, and prognosis of patients. The piloted data form is provided in Appendix B.1.
Risk of bias assessment
For methodological quality assessment of observational studies, which included cross-sectional studies, cohort studies, and case-control studies, two different assessment tools were utilized to determine how well each individual study addressed the potential risk of bias.
All existing cohort studies and case-control studies were assessed using the Newcastle-Ottawa Scale by Wells et al. [14] and cross-sectional studies in the present review were analyzed using the The Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Analytical Cross-Sectional Studies [15].
Results
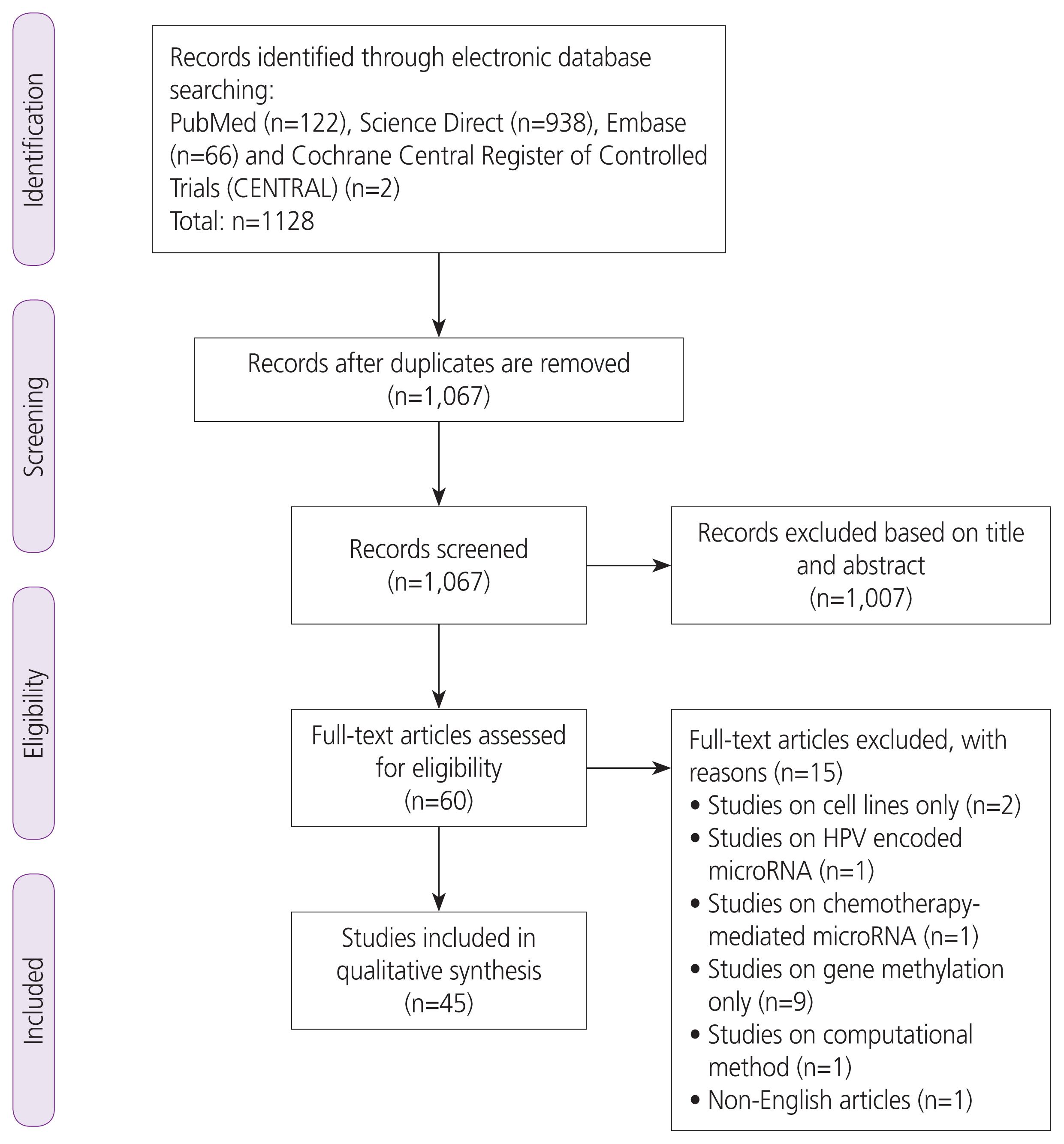
The study selection process is summarized in Fig. 1 (PRISMA Flow Chart). Our initial search identified 1,128 potentially relevant articles. We included 62 articles after screening the titles and abstracts. Seventeen articles were excluded after further scrutiny. A complete list of the excluded studies is available from the authors.
Characteristics of selected studies
In total, 45 articles (22 case-control studies, 4 prospective cohort studies, and 19 cross-sectional studies) were included in this systematic review. The studies were carried out across several continents, namely Asia (n=30), Europe (n=11), South America (n=3), and Africa (n=1). Twenty-five studies were from China, four studies from the Netherlands [16-19], three studies from Portugal [20-22], two studies each from India [23,24] and Mexico [25,26], and one study each from Thailand, Japan, Russia, Italy, Hungary, Czech Republic, Sweden, Brazil, and Nigeria [27-35]. The main characteristics of the selected studies are listed in Table 2.
Dysregulated miRNAs in cervical carcinogenesis
1. Upregulated miRNAs
Approximately 82 individual miRNAs were found to be significant in differentiating the stages of cervical carcinogenesis. The significantly upregulated miRNAs included miR-21 and miR-15 in LSIL, high-grade squamous intraepithelial lesions (HSILs), and cervical cancer in plasma serum, cervical exfoliated cells, and cervical tissue samples. miR-21 expression was found to be predominantly detected in the tumor-associated stroma of squamous cell carcinomas [27]. miR-21 was also found to be correlated with advanced cervical cancer lesions with progressively increased expression in more severe clinical manifestations [24].
Other miRNAs such as miR-196, miR-20, miR-155, miR-27, miR-200, miR-9, miR-146a, miR-193, miR-148, miR-10, miR-132, miR-141, and miR-93 were found to be upregulated in cervical cancer as compared to normal plasma serum, cervical mucus, and cervical tissue samples in studies conducted in Europe, Nigeria, Mexico and mainly in Asia [16-21,36-38]. miR-141 expression levels were found to be significantly higher in younger participants than in older cohorts [39].
In groups comparing expression levels of LSIL to HSIL, upregulated miRNAs include miR-20, miR-155, miR-27, and miR-16 in plasma serum and cervical tissue samples [31,40]. Interestingly, miR-200 was upregulated in cervical cell samples but downregulated in serum samples from patient groups comparing LSIL to HSIL [35]. In groups comparing HSIL to cervical cancer stages, miR-155, miR-27, miR-196, miR-200, miR-222, miR-9, miR-146a, miR-1, miR-17, miR-106, miR-148, miR-10, miR-132, and miR-205 were upregulated. miR-205 has also been shown to have a higher specificity than HPV testing in predicting the absence of HSIL in exfoliated cell samples [33].
2. Downregulated miRNAs
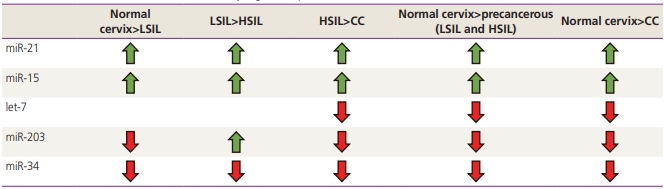
The significantly downregulated miRNAs included, let-7, miR-203, and miR-34 in LSIL, HSIL, and cervical cancer compared to controls. Furthermore, miR-34 is predominantly downregulated in HSIL compared to LSIL [31,41].
Other miRNAs, such as miR-29, miR-20, miR-125, miR-199, miR-23b, miR-99a, miR-126, miR-145, miR-149, miR-143, and miR-26a were downregulated in plasma serum, cervical exfoliated cells, and cervical tissue samples [16,19,21,29,31,42,43] miR-126 was found to be upregulated in cervical mucus, but downregulated in cervical tissues in two respective studies [28,29]. In particular, miR-20 was found to have a higher detection performance in LSIL and HSIL than in cervical cancer samples [39]. miR-146 was also found to have a higher expression in plasma serum than in cervical cells [35]. The expression of the five most common miRNAs and their dysregulation patterns are shown in Table 3.
miRNAs in non-conventional sample types
1. Cervical mucus samples
A total of four miRNAs, miR-126 miR-20, miR-451, and miR-144, were found to be significantly expressed in the cervical mucus samples. In particular, miR-451 and miR-144 were found to be significantly upregulated in cervical mucus samples [28]. Interestingly, miR-126 was upregulated in cervical mucus but downregulated in cell samples of cervical cancer patients compared to control patients [28,29]. Table 4 shows the miRNAs detected in the cervical mucus samples.
2. Plasma serum samples
A total of 11 miRNAs were investigated in serum samples from four studies [35,42,44,45]. Nine miRNAs, namely miR-21, miR-146, miR-155, miR-200, miR-34, miR-let-7, miR-182, miR-145, and miR-1266 were found to be differentially expressed in the cells, tissue, and serum samples of patients with abnormal cervical smears. Two miRNAs, namely miR-214 and miR-466, were found to be significantly expressed only in serum samples [44,46].
3. MiRNAs and HPV infection
MiR-21 was upregulated in HPV-positive samples compared to HPV-negative samples, while miR-3156-3p and miR-155-5p expression were lower in HPV-positive cervical cancer [27,47]. Several studies have found correlations between the expression of miRNAs and HPV E6 and E7 viral genes. A positive correlation was observed between miR-25 and miR-21 with HPV E7 and E6, respectively, indicating that these miRNAs are specific to these viral proteins [24,48]. A negative correlation was found between miR-129-5p, miR-409-3p, and let-7a with the level of HPV E6/E7 [24,32,41]. HPV-positive cervical mucus samples demonstrated upregulation of miR-126-3p, miR-20b-5p, miR-451a, and miR-144-3p, respectively [28].
4. Risk of bias assessment
The quality of the case-control and cohort studies was evaluated using the Newcastle-Ottawa Scale. The overall quality of the case-control studies was not outstanding, as 50% (n=11) of the studies reviewed were scored as good quality. For most case-control studies, the authors failed to provide or did not mention a suitable comparability of study design between the cases and controls. Most studies enrolled healthy patients (normal controls) through clinical settings that were convenient to investigators. Only three studies recruited normal and healthy participants through community screenings, which generally contributed to higher scoring [16,17,49]. Similar mediocre results were achieved during the assessment of cohort studies, with half of the studies scored as good quality [44,46]. For cohort studies, there was a loss of follow-up noted in one study conducted by Wang et al. [50]. High-quality studies were prioritized based on this scoring system.
For the 19 cross-sectional studies, the quality of the studies was analyzed using the JBI Critical Appraisal Checklist for Analytical Cross-Sectional Studies [15]. Most of the studies failed to identify any confounding factors that may influence the expression levels of miRNAs; only two studies analyzed sociodemographic factors [31,40]. A lack of clear definition was observed for the inclusion and exclusion criteria in a total of nine studies. Most studies utilized appropriate statistical analyses; however, four studies did not provide a clear explanation of the statistical tests used [41,50-52]. All 19 studies were ultimately included in the present study. Supplementary Table 1-3, Fig. 1 show the quality assessment for case-control, cross-sectional, and cohort studies.
Discussion
1. Summary of main results
A systematic review was performed to identify the role of miRNAs as biomarkers in the progression of cervical precancerous lesions. The results of the systematic analysis identified the most prominent dysregulated miRNAs. Among the upregulated mRNAs, miR-21 has been shown to be consistently upregulated progressively from normal cervical to worsening cervical lesion stages in both cell and serum samples [18,24,27,35,43,51,53]. miR-21 is a key miRNA that is found to be increased in many diseased states, such as inflammation, cardiac injuries, and various tumors in mammalian tissues [36,54]. Apart from cervical cancer, miR-21 has been shown to have oncogenic effects in both solid tumors such as liver cancer, lung cancer, and non-solid tumors such as chronic lymphocytic leukemia [36]. It has been shown to be expressed in hematopoietic cells of the immune system, which respond to tumor progression, and is linked to greater immune cell activation, supporting our findings that miR-21 is an oncogenic miRNA [54]. Moreover, there is a strong correlation between upregulated miR-21 and gene hypomethylation in the regulation of cancer genes and poor survival rate in cancer patients [38]. It was also noted to be particularly high in advanced cancers with severe manifestations [24]. Evidently, miR-21 is a reliable, highly profiled miRNA that is commonly overexpressed in cervical cancer, making it a promising biomarker for tumor detection.
Among the downregulated miRNAs, miR-34, let-7, and miR-203 were proven to be significantly downregulated in LSIL, HSIL, and cervical cancer across multiple studies [21-24,31-34]. miR-34 and miR-21 were also found to be more specific than HPV testing in differentiating LSIL from HSIL and may provide more accurate detection results [53]. The dysregulation of these four miRNAs was observed to be an early onset event in the development of cervical cancer. It has also been reported that miR-34 has a synergistic effect with p53, a well-known tumor suppressor, further reinforcing its regulatory role in carcinogenesis [37]. Again, miR-34 was found to be upregulated in thyroid and liver cancer but downregulated in cervical, breast, and lung cancer, suggesting that the individual miRNAs may have different expression levels in various cell types [37].
It was discovered that miRNAs in cervical mucus have higher detection accuracies for detecting adenocarcinoma than conventional cytological methods [55]. However, significant results were only found at late stages of precancerous lesions (HSIL/CIN II-III), suggesting that miRNAs in cervical mucus could be a potential biomarker for HSIL and cervical cancer [28].
It was also shown that miRNAs maintain their stability despite being subjected to harsh conditions [56]. Wang et al. [42] confirmed that the expression levels of miRNAs were consistently similar in both plasma serum and cervical biopsy tissue, which further suggests that plasma serum reflects the true miRNA levels with less painful methods. Due to the low cost and relatively less invasive nature of phlebotomy, a blood-based test for cervical cancer would be an appealing option [57]. If proven successful, the detection of cervical-specific miRNAs will be a cost-effective and convenient option for patients who concurrently require blood tests for other health issues [57]. It would also allow for further community screening, which reduces the late detection rate of cervical cancer.
Currently, the available data on serum-based and cervical mucus-based tests are limited, despite their suitability for widespread use [58]. The comparability of the sensitivities and specificities of miRNAs in body fluids as compared to biopsy tissues is uncertain. Hence, more research is needed to directly compare these sampling methods and their efficacy.
The review found a correlation between miRNA expression and the presence of HPV infection in multiple studies. Many miRNAs exhibit dysregulated expression in HPV-positive patients. HPV 16 positivity was correlated with the expression of miR-27 and miR-34 from LSIL to HSIL [59]. Multiple HPV genotypes have been found to act synergistically in cervical carcinogenesis [31].
One study discovered that the viral genes E6 and E7 could both enhance the levels of miR-92a, but only viral E7 was able to upregulate the expression of miR-25 [48]. This demonstrated that certain oncoproteins have specific targeted miRNAs and different abilities to navigate HPV infection in cervical cells.
2. Study limitations
This systematic review has several limitations. First, the variation in sample sizes across selected studies may have affected the results of some miRNAs. Some studies have hugely disproportionate sample sizes in each category, which may have impacted the precision of the data. There was considerable heterogeneity, and hence, a meta-analysis was not possible. However, most of the included studies had sufficient sample sizes and data to draw valid conclusions.
The quality of certain included studies varied because the primary aim was not to investigate the correlation of miRNA expression with different cervical lesions. However, all included studies provided adequate data on miRNA expression levels in various cervical lesions. The quality of collected samples varied, as a few studies collected both cervical cancer cells and adjacent healthy cervical cells from the same patient. It is recommended that future studies obtain diseased and healthy cells from two different patient groups, respectively, for more accurate results.
3. Implications for clinical practice
The overwhelming amount of data available has validated that the ubiquitously aberrant expression of miRNAs is closely associated with the pathogenesis and progression of various human malignancies. This review presents significantly dysregulated miRNAs in cervical carcinogenesis with their dynamic expression changes and ability to detect viral persistency, risk prediction of low-grade lesions (CIN 2) to high-grade lesions (CIN 3), and progression of CIN 3 to cancer. Their ability to discriminate HSILs from non-dysplastic lesions has potential implications in early diagnosis and reducing overtreatment of otherwise regressive early preinvasive lesions. As most cervical cancers, especially in developing countries, are detected at an advanced stage, there is potential value of miRNAs as diagnostic and prognostic biomarkers in advanced intraepithelial lesions and cancer. miRNAs are relatively easy to measure under laboratory conditions owing to their considerably greater stability as compared to other RNAs. The findings also suggest that less invasive methods of sampling can be adopted, such as through plasma serum or cervical mucus, are feasible, albeit limited available knowledge on their clinical applications.
4. Future research
Future studies on miRNA profiling should be conducted on different body fluids to provide the highest detection accuracy and convenience for patients. However, there is a need for standardization to obtain repeatability and comparability of the test results. It is therefore paramount to have extensive clinical trials that will enable the development of algorithms before miRNA profiling can be utilized as a detailed fingerprint of a cell’s dysregulation at the molecular level.
Conclusions
In conclusion, our study identified significant dysregulated miRNAs in cervical carcinogenesis with their dynamic expression changes and ability to detect viral persistency, risk prediction of low-grade lesions (CIN 2) to high-grade lesions (CIN 3), and the progression of CIN 3 to cancer. Their ability to discriminate HSIL from non-dysplastic lesions. This has potential implications for early diagnosis and reducing overtreatment of otherwise regressive early preinvasive lesions.







")











